

Stroke impairment categories: A new way to classify the effects of stroke based on stroke-related impairments
- PMID: 33131321
- PMCID: PMC7944424
- DOI: 10.1177/0269215520966473
Stroke impairment categories: A new way to classify the effects of stroke based on stroke-related impairments
Abstract
Objective: To create a classification system based on stroke-related impairments.
Data source: All adults with stroke admitted for at least 72 hours in England, Wales and Northern Ireland from July 2013 to July 2015 extracted from the Sentinel Stroke National Audit Programme.
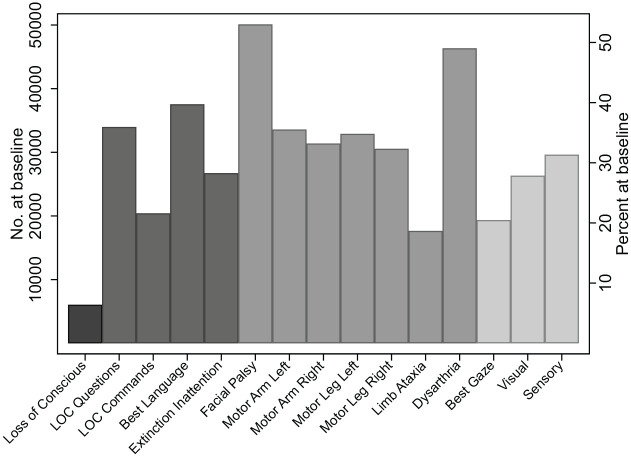
Analysis: Impairments were defined using the National Institute of Health Stroke Scale scores at admission. Common combinations of impairments were identified based on geometric coding and expert knowledge. Validity of the classification was assessed using standard descriptive statistics to report and compare patients' characteristics, therapy received and outcomes in each group.
Results: Data from 94,905 patients were extracted. The items of the National Institute of Health Stroke Scale (on admission) were initially grouped into four body systems: Cognitive, Motor, Sensory and Consciousness. Seven common combinations of these impairments were identified (in order of stroke severity); Patients with Loss of Consciousness (n = 6034, 6.4%); those with Motor + Cognitive + Sensory impairments (n = 28,226, 29.7%); Motor + Cognitive impairments (n = 16,967, 17.9%); Motor + Sensory impairments (n = 9882, 10.4%); Motor Only impairments (n = 20,471, 21.6%); Any Non-Motor impairments (n = 7498, 7.9%); and No Impairments (n = 5827, 6.1%). There was a gradation of age, premorbid disability, mortality and disability on discharge. People with the most and least severe categories were least likely to receive therapy, and received least therapy (-20 minutes/day of stay) compared to -35 minutes/day of stay for the moderately severe categories.
Conclusions: A classification system of seven Stroke Impairment Categories has been presented.
Keywords: Stroke; disability; length of stay; occupational therapy; physiotherapy; psychology; rehabilitation; speech and language therapy.
Conflict of interest statement
Figures
References
-
- Bamford J, Sandercock P, Dennis M, et al.. Classification and natural-history of clinically identifiable subtypes of cerebral infarction. Lancet 1991; 337: 1521–1526. - PubMed
-
- Bamford JM. The role of the clinical examination in the subclassification of stroke. Cerebrovasc Dis 2000; 10: 2–4. - PubMed
-
- Sanchez-Blanco I, Ochoa-Sangrador C, Lopez-Munain L, et al.. Predictive model of functional independence in stroke patients admitted to a rehabilitation programme. Clin Rehabil 1999; 13: 464–475. - PubMed
-
- Tyson ST, Turner GF. Southampton stroke audit: assessing service quality. Br J Occup Ther 1999; 6: 227–232.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
