

Right ventricular failure in septic shock: characterization, incidence and impact on fluid responsiveness
- PMID: 33131508
- PMCID: PMC7603714
- DOI: 10.1186/s13054-020-03345-z
Right ventricular failure in septic shock: characterization, incidence and impact on fluid responsiveness
Abstract
Objective: Incidence of right ventricular (RV) failure in septic shock patients is not well known, and tricuspid annular plane systolic excursion (TAPSE) could be of limited value. We report the incidence of RV failure in patients with septic shock, its potential impact on the response to fluids, as well as TAPSE values.
Design: Ancillary study of the HEMOPRED prospective multicenter study includes patients under mechanical ventilation with circulatory failure.
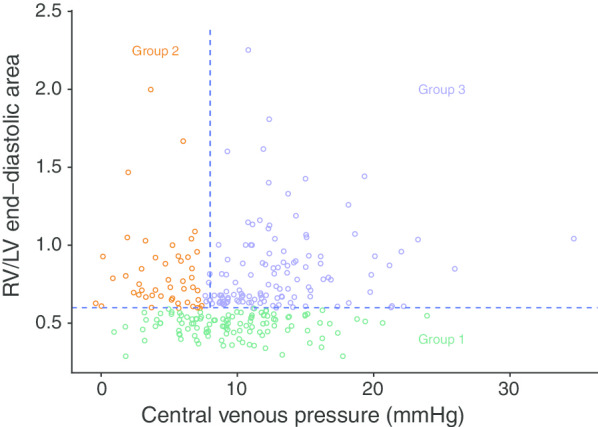
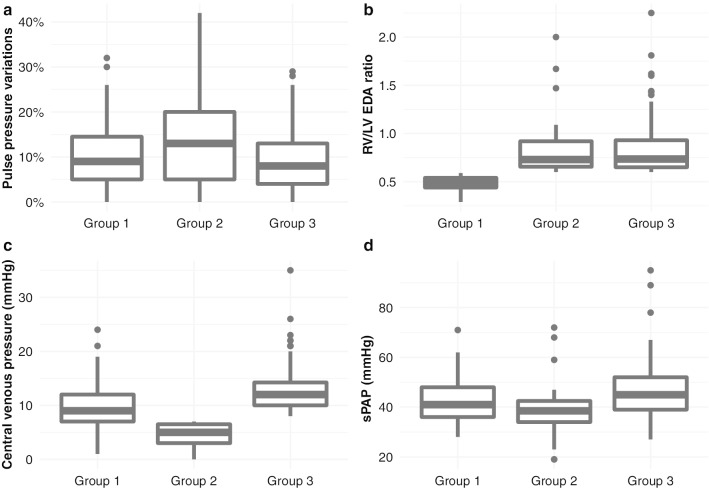
Setting: This is a multicenter intensive care unit study PATIENTS: Two hundred and eighty-two patients with septic shock were analyzed. Patients were classified in three groups based on central venous pressure (CVP) and RV size (RV/LV end-diastolic area, EDA). In group 1, patients had no RV dilatation (RV/LVEDA < 0.6). In group 2, patients had RV dilatation (RV/LVEDA ≥ 0.6) with a CVP < 8 mmHg (no venous congestion). RV failure was defined in group 3 by RV dilatation and a CVP ≥ 8 mmHg. Pulse pressure variation (PPV) was systematically recorded.
Interventions: None.
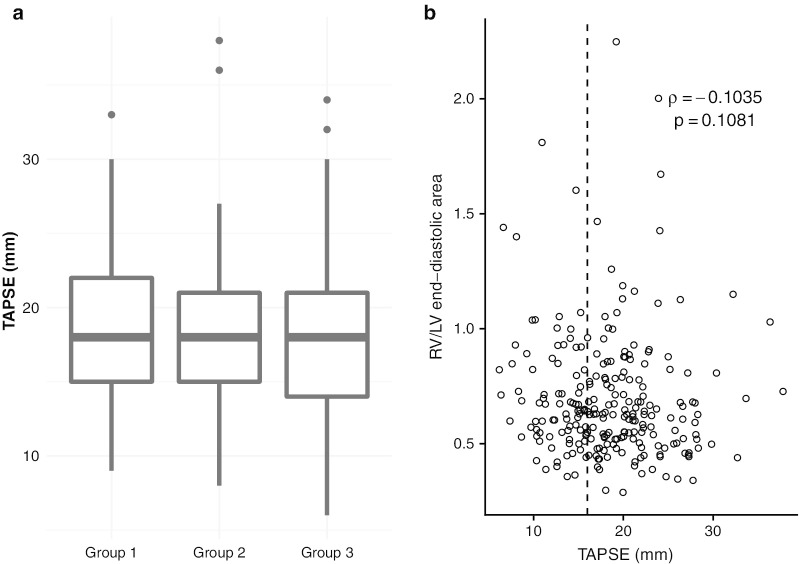
Measurements and main results: In total, 41% of patients were in group 1, 17% in group 2 and 42% in group 3. A correlation between RV size and CVP was only observed in group 3. Higher RV size was associated with a lower response to passive leg raising for a given PPV. A large overlap of TAPSE values was observed between the 3 groups. 63.5% of patients with RV failure had a normal TAPSE.
Conclusions: RV failure, defined by critical care echocardiography (RV dilatation) and a surrogate of venous congestion (CVP ≥ 8 mmHg), was frequently observed in septic shock patients and negatively associated with response to a fluid challenge despite significant PPV. TAPSE was unable to discriminate patients with or without RV failure.
Keywords: Central venous pressure; Critical care echocardiography; Fluid responsiveness; Right ventricular failure; TAPSE.
Conflict of interest statement
None.
Figures

Comment in
-
Comments on "Right ventricular failure in septic shock: characterization, incidence and impact on fluid responsiveness": which parameter to assess right ventricular failure and venous congestion?Crit Care. 2021 Apr 9;25(1):136. doi: 10.1186/s13054-021-03473-0. Crit Care. 2021. PMID: 33836816 Free PMC article. No abstract available.
References
-
- Harjola V-P, Mebazaa A, Čelutkienė J, et al. Contemporary management of acute right ventricular failure: a statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur J Heart Fail. 2016;18:226–241. doi: 10.1002/ejhf.478. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
