

Olfactory Bulb MRI and Paranasal Sinus CT Findings in Persistent COVID-19 Anosmia
- PMID: 33132007
- PMCID: PMC7571972
- DOI: 10.1016/j.acra.2020.10.006
Olfactory Bulb MRI and Paranasal Sinus CT Findings in Persistent COVID-19 Anosmia
Abstract
Background and purpose: There is limited literature consisting of case reports or series on olfactory bulb imaging in COVID-19 olfactory dysfunction. An imaging study with objective clinical correlation is needed in COVID-19 anosmia in order to better understand underlying pathogenesis.
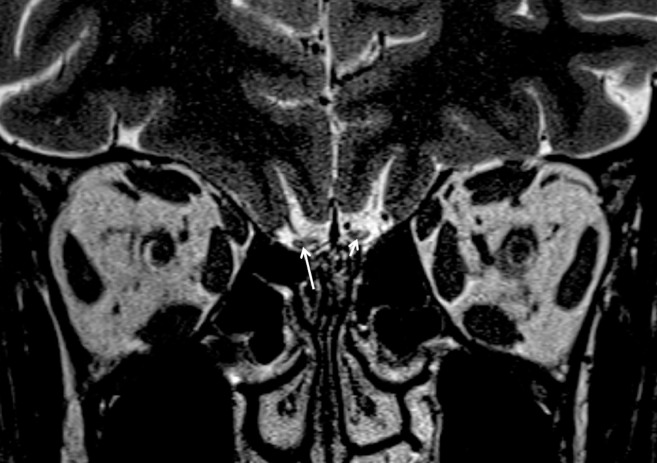
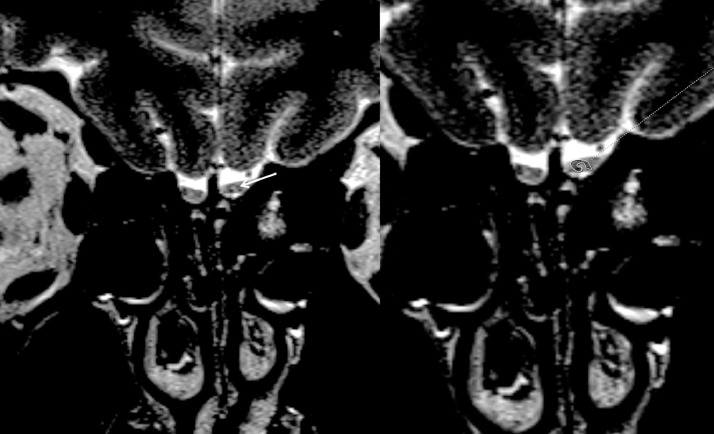
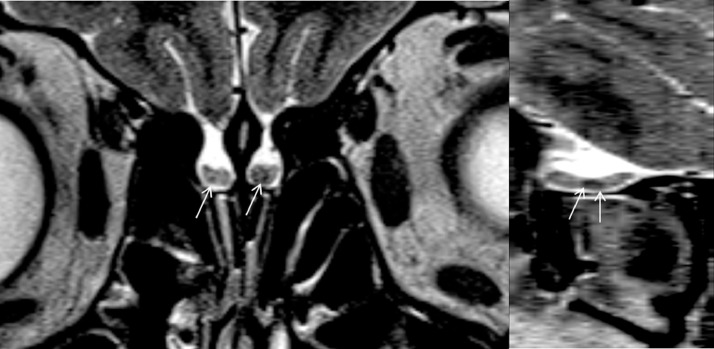
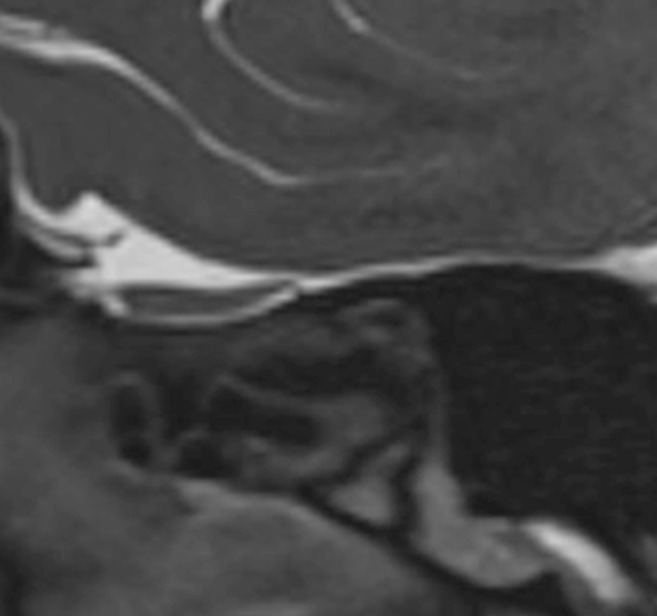
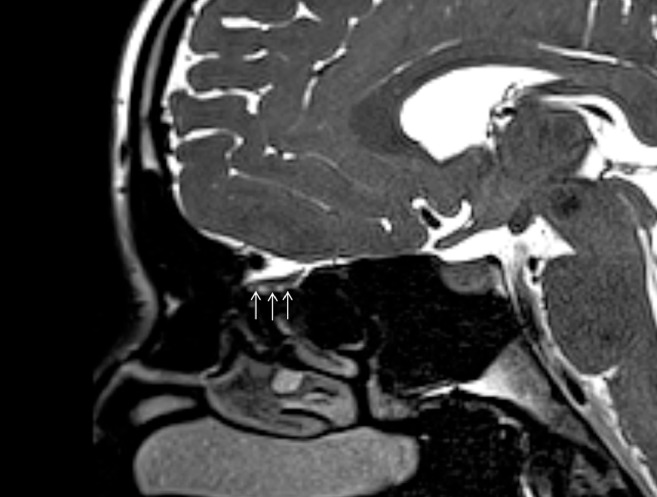
Material and methods: We evaluated 23 patients with persistent COVID-19 olfactory dysfunction. Patients included in this study had a minimum 1-month duration between onset of olfactory dysfunction and evaluation. Olfactory functions were evaluated with Sniffin' Sticks Test. Paranasal sinus CTs and MRI dedicated to olfactory nerves were acquired. On MRI, quantitative measurements of olfactory bulb volumes and olfactory sulcus depth and qualitative assessment of olfactory bulb morphology, signal intensity, and olfactory nerve filia architecture were performed.
Results: All patients were anosmic at the time of imaging based on olfactory test results. On CT, Olfactory cleft opacification was seen in 73.9% of cases with a mid and posterior segment dominance. 43.5% of cases had below normal olfactory bulb volumes and 60.9% of cases had shallow olfactory sulci. Of all, 54.2% of cases had changes in normal inverted J shape of the bulb. 91.3% of cases had abnormality in olfactory bulb signal intensity in the forms of diffusely increased signal intensity, scattered hyperintense foci or microhemorrhages. Evident clumping of olfactory filia was seen in 34.8% of cases and thinning with scarcity of filia in 17.4%. Primary olfactory cortical signal abnormality was seen in 21.7% of cases.
Conclusion: Our findings indicate olfactory cleft and olfactory bulb abnormalities are seen in COVID-19 anosmia. There was a relatively high percentage of olfactory bulb degeneration. Further longitudinal imaging studies could shed light on the mechanism of olfactory neuronal pathway injury in COVID-19 anosmia.
Keywords: Anosmia; COVID-19; MRI; Olfactory bulb; Olfactory cleft; Olfactory nerve; Paranasal sinus CT.
Copyright © 2020 The Association of University Radiologists. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest None to declare.
Figures


References
-
- Hoang M.P., Kanjanaumporn J., Aeumjaturapat S. Olfactory and gustatory dysfunctions in COVID-19 patients: a systematic review and meta-analysis. Asian Pac J Allergy Immunol. 2020;38:162–169. - PubMed
-
- Duprez T.P., Rombaux P. Imaging the olfactory tract (cranial nerve #1) Eur J Radiol. 2010;74:288–298. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
