

Hydrocolloid dressing improves wound healing by increasing M2 macrophage polarization in mice with diabetes
- PMID: 33132433
- PMCID: PMC7548260
- DOI: 10.18999/nagjms.82.3.487
Hydrocolloid dressing improves wound healing by increasing M2 macrophage polarization in mice with diabetes
Abstract
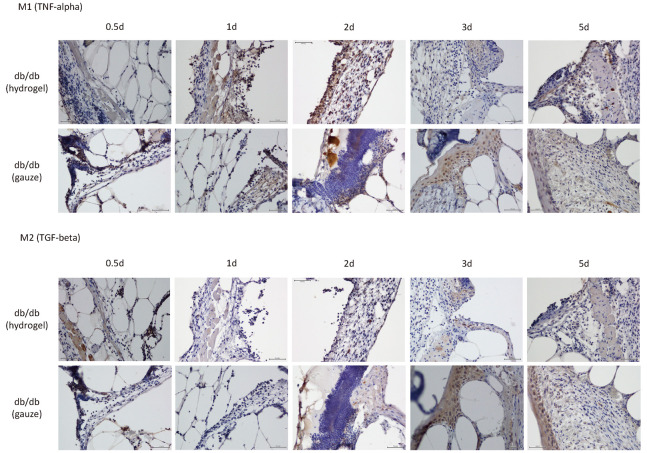
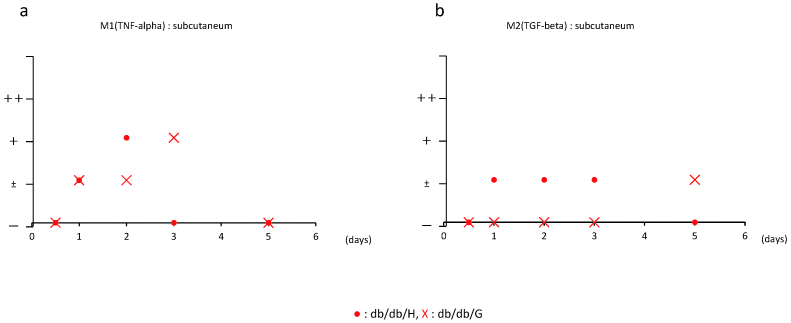
Impaired wound healing is one of the most common complications of diabetes, and is known to be caused by multiple complicated factors. For instance, impaired angiogenesis, neuropathy, and hyperglycemia all function to delay subsequent wound closure. Alternatively, moist wound healing, which provides an appropriate environment for wounds, was reported to permit rapid healing by managing wound exudate. Accordingly, wound dressing materials that facilitate moist healing have been developed. The present study sought to clarify the effects of wound dressing material for moist healing of diabetic wounds, in terms of the dynamics of angiogenic factors and macrophages, using a mouse model of naturally occurring diabetes. Wounds with full-thickness skin defects were inflicted on the backs of mice and covered with dressing materials of hydrogel or gauze (control), which were retained for 3, 5, 7, 10, or 14 days following wound generation. During this time, the localization of neutrophils, fibroblasts and macrophages as well as the expression of vascular endothelial growth factor (VEGF) in the wounds and surrounding areas was observed each day. Healing clearly occurred in the hydrogel group with an increase in neutrophils and the angiogenic factor, VEGF. Moreover, the use of hydrogel resulted in a rapid rise in M1 macrophages, which appeared in the early stage of the injury, as well as rapid subsequent appearance of M2 macrophages. Thus, herein, we demonstrate that the formation of a moist environment via wound dressing material effectively improves diabetic wound healing.
Keywords: M2 macrophage; diabetic mice; hydrocolloid dressing; wound healing.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures




Similar articles
-
Novel hydrocolloid-sheet as wound dressing to stimulate healing-impaired wound healing in diabetic db/db mice.Biomed Mater Eng. 2012;22(5):301-10. doi: 10.3233/BME-2012-0720. Biomed Mater Eng. 2012. PMID: 23023147
-
Suppressed recruitment of alternatively activated macrophages reduces TGF-β1 and impairs wound healing in streptozotocin-induced diabetic mice.Biomed Pharmacother. 2015 Mar;70:317-25. doi: 10.1016/j.biopha.2014.10.020. Epub 2014 Oct 31. Biomed Pharmacother. 2015. PMID: 25677561
-
Keratin Scaffolds Containing Casomorphin Stimulate Macrophage Infiltration and Accelerate Full-Thickness Cutaneous Wound Healing in Diabetic Mice.Molecules. 2021 Apr 27;26(9):2554. doi: 10.3390/molecules26092554. Molecules. 2021. PMID: 33925737 Free PMC article.
-
Therapeutic Properties of M2 Macrophages in Chronic Wounds: An Innovative Area of Biomaterial-Assisted M2 Macrophage Targeted Therapy.Stem Cell Rev Rep. 2025 Feb;21(2):390-422. doi: 10.1007/s12015-024-10806-3. Epub 2024 Nov 18. Stem Cell Rev Rep. 2025. PMID: 39556244 Review.
-
An investigation of the benefits of Aquacel Hydrofibre wound dressing.Br J Nurs. 1999 May 27-Jun 9;8(10):676-7, 680. doi: 10.12968/bjon.1999.8.10.6607. Br J Nurs. 1999. PMID: 10624199 Review.
Cited by
-
Biomedical materials for wound dressing: recent advances and applications.RSC Adv. 2023 Feb 13;13(8):5509-5528. doi: 10.1039/d2ra07673j. eCollection 2023 Feb 6. RSC Adv. 2023. PMID: 36793301 Free PMC article. Review.
-
Wound Healing Performance in a Moist Environment of Crystalline Glucose/Mannose Film as a New Dressing Material Using a Rat Model: Comparing with Medical-Grade Wound Dressing and Alginate.Pharmaceuticals (Basel). 2023 Oct 30;16(11):1532. doi: 10.3390/ph16111532. Pharmaceuticals (Basel). 2023. PMID: 38004398 Free PMC article.
-
Narrative Review of the Use of Hydrocolloids in Dermatology: Applications and Benefits.J Clin Med. 2025 Feb 18;14(4):1345. doi: 10.3390/jcm14041345. J Clin Med. 2025. PMID: 40004874 Free PMC article. Review.
-
Effect of hydrocolloid dressing combined with continuous nursing intervention on patients with permanent ostomy.BMC Surg. 2025 Aug 2;25(1):335. doi: 10.1186/s12893-025-03058-6. BMC Surg. 2025. PMID: 40753380 Free PMC article.
-
Natural and Synthetic Polymeric Biomaterials for Application in Wound Management.J Funct Biomater. 2023 Sep 3;14(9):455. doi: 10.3390/jfb14090455. J Funct Biomater. 2023. PMID: 37754869 Free PMC article. Review.
References
-
- Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011;94(3):311–321. - PubMed
-
- Greenhalgh DG. Wound healing and diabetes mellitus. Clin Plast Surg. 2003;30(1):37–45. - PubMed
-
- Peters EJ, Lipsky BA. Diagnosis and management of infection in the diabetic foot. Med Clin North Am. 2013;97(5):911–946. - PubMed
-
- Noor S, Khan RU, Ahmad J. Understanding Diabetic Foot Infection and its Management. Diabetes Metab Syndr. 2017;11(2):149–156. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources