

Combination of Inferior Vena Cava Diameter, Hepatic Venous Flow, and Portal Vein Pulsatility Index: Venous Excess Ultrasound Score (VEXUS Score) in Predicting Acute Kidney Injury in Patients with Cardiorenal Syndrome: A Prospective Cohort Study
- PMID: 33132560
- PMCID: PMC7584837
- DOI: 10.5005/jp-journals-10071-23570
Combination of Inferior Vena Cava Diameter, Hepatic Venous Flow, and Portal Vein Pulsatility Index: Venous Excess Ultrasound Score (VEXUS Score) in Predicting Acute Kidney Injury in Patients with Cardiorenal Syndrome: A Prospective Cohort Study
Abstract
Background: Fluid overload is deleterious in critically ill patients. It can lead to venous congestion, thereby increasing venous pressure, theoretically increasing the backpressure, and thereby reducing renal blood flow. Venous congestion thus can be an important contributor to acute kidney injury (AKI), with no validated tools to objectively identify venous congestion bedside.
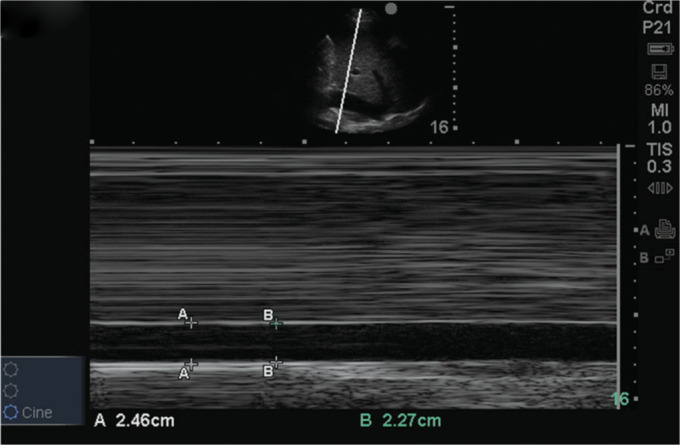
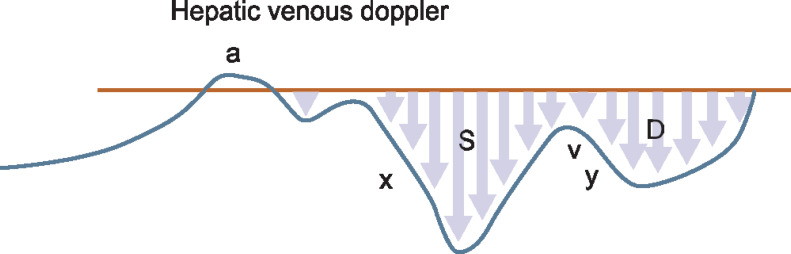
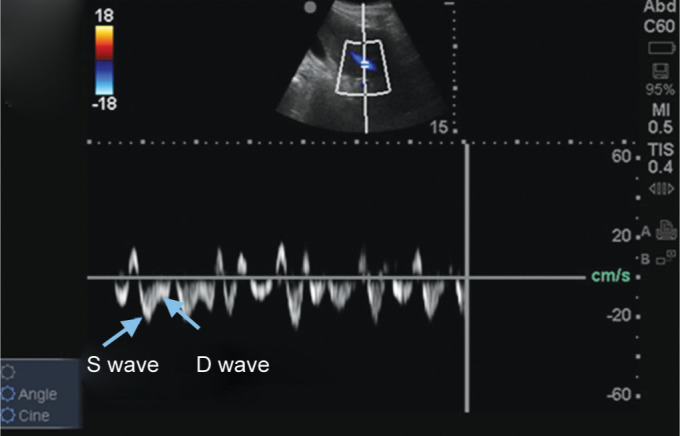
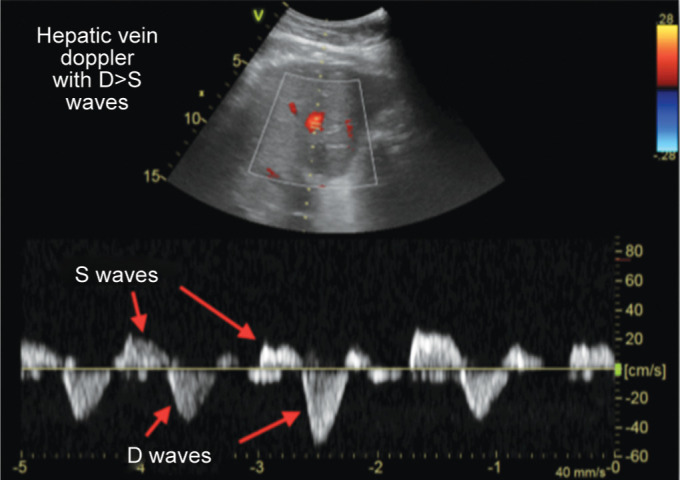
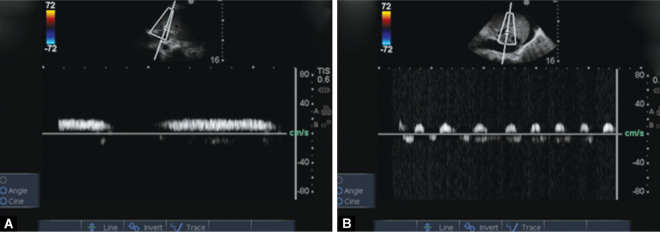
Materials and methods: Patients above 18 years admitted in ICU with a provisional diagnosis of cardiorenal syndrome were included in the study. Those with inadequate window, inferior vena cava (IVC) thrombus, and known case of cirrhosis with portal hypertension were excluded from the study. Patients underwent ultrasound examination with serial determination till AKI resolved or patient is initiated on dialysis. Venous excess ultrasound score (VEXUS) comprising inferior vena cava, hepatic vein waveform, and portal vein pulsatility was assessed.
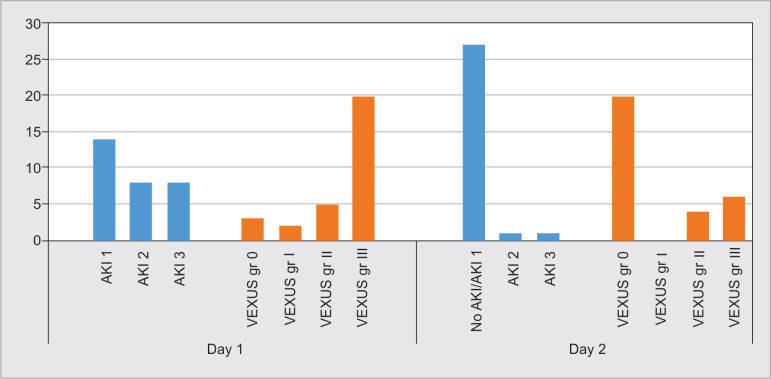
Results: Thirty patients were enrolled for the study. The mean age was 59.53 ± 16.47 with 21 (70%) males. Mean sequential organ failure assessment (SOFA) score was 5.03 ± 1.97. Fourteen patients (46.7%) were in AKI stage 1, while eight patients (26.7%) were in AKI stage 2 and stage 3 each. Twenty patients (66.7%) had VEXUS grade III. Resolution of AKI injury showed significant correlation with improvement in VEXUS grade (p value 0.003). Similarly, there was significant association between changes in VEXUS grade and fluid balance (p value 0.006). There was no correlation between central venous pressure (CVP), left ventricular function, and right ventricular function with change in VEXUS grade.
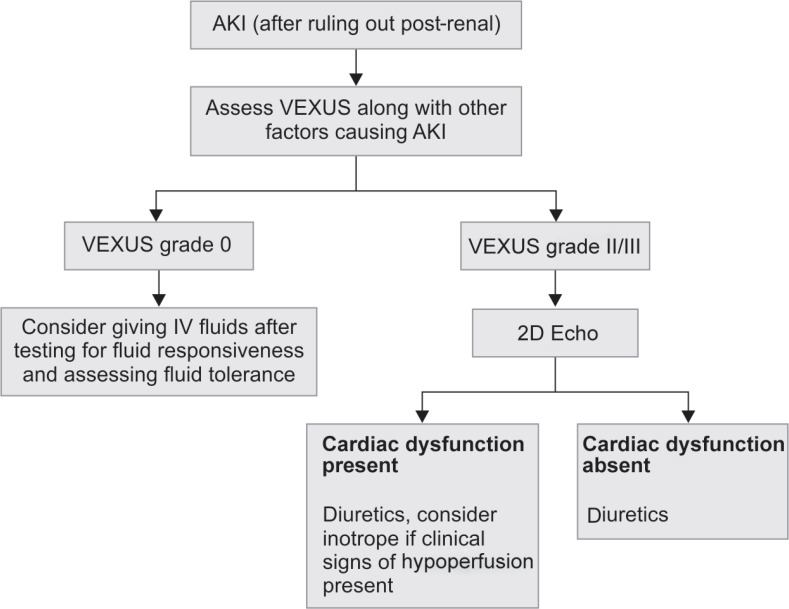
Conclusion: The study shows that a combined grading of IVC, hepatic vein, and portal vein might reliably demonstrate venous congestion and aid in the clinical decision to perform fluid removal.
How to cite this article: Bhardwaj V, Vikneswaran G, Rola P, Raju S, Bhat RS, Jayakumar A, et al. Combination of Inferior Vena Cava Diameter, Hepatic Venous Flow, and Portal Vein Pulsatility Index: Venous Excess Ultrasound Score (VEXUS Score) in Predicting Acute Kidney Injury in Patients with Cardiorenal Syndrome: A Prospective Cohort Study. Indian J Crit Care Med 2020;24(9):783-789.
Keywords: Acute kidney injury; Fluid balance; Portal vein pulsatility; Venous congestion; Volume overload.
Copyright © 2020; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures
References
-
- Guinot PG, Abou-Arab O, Longrois D, Dupont H. Right ventricular systolic dysfunction and vena cava dilatation precede alteration of renal function in adult patients undergoing cardiac surgery: an observational study. Eur J Anaesthesiol. 2015;32(8):535–542. doi: 10.1097/EJA.0000000000000149. DOI: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical