

State of Personal Protective Equipment Practice in Indian Intensive Care Units amidst COVID-19 Pandemic: A Nationwide Survey
- PMID: 33132565
- PMCID: PMC7584819
- DOI: 10.5005/jp-journals-10071-23550
State of Personal Protective Equipment Practice in Indian Intensive Care Units amidst COVID-19 Pandemic: A Nationwide Survey
Abstract
Background: Optimal personal protective equipment (PPE) preparedness is key to minimize healthcare workers (HCW) infection with COVID-19. This two-phase survey evaluated PPE preparedness (adherence to Ministry of Health India (MoH) PPE-recommendations; HCW-training; PPE-inventory; PPE-breach management) in Indian intensive care units (ICU).
Materials and methods: The phase 1 survey was distributed electronically to intensivists from 481 Indian hospitals between March 25, 2020, and April 06, 2020, as part of a multinational survey. Phase 2 was repeated in 320 Indian hospitals between April 20, 2020, and April 30, 2020.
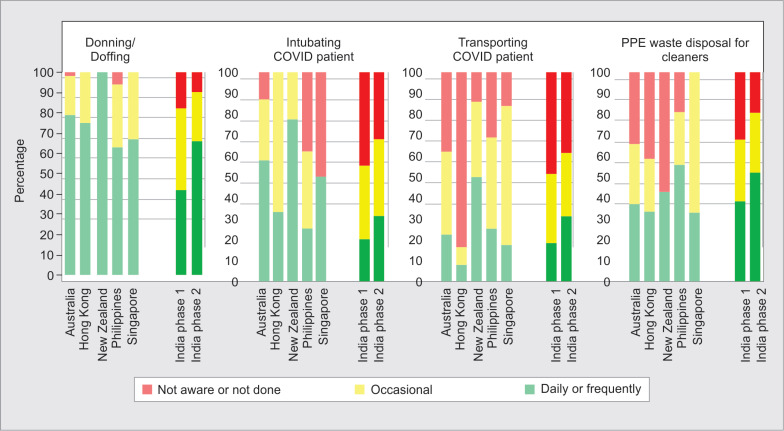
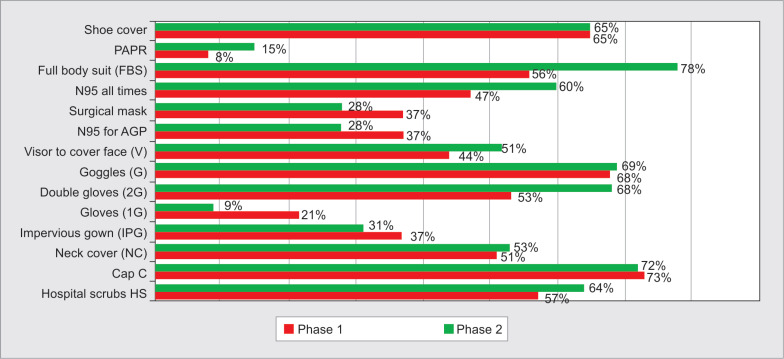
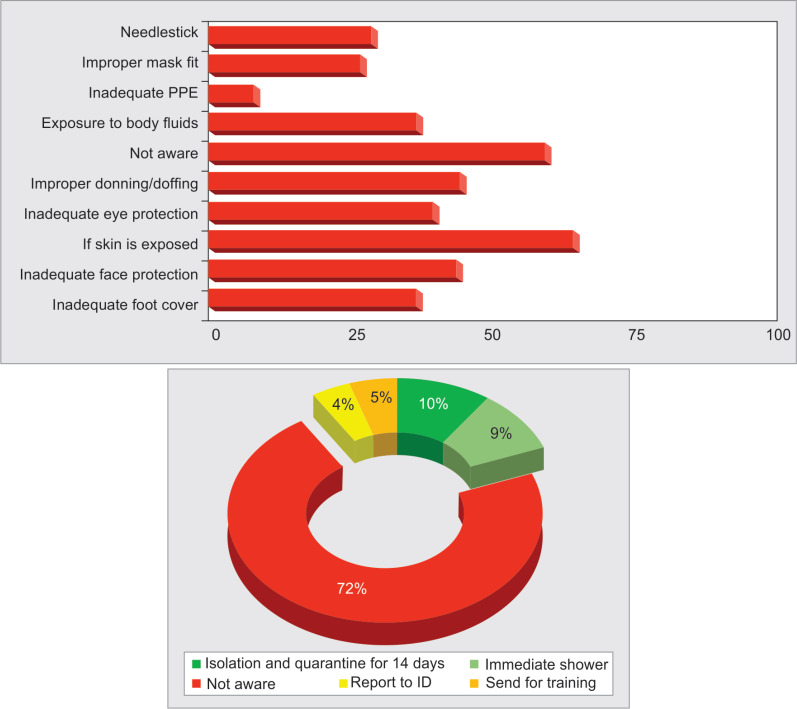
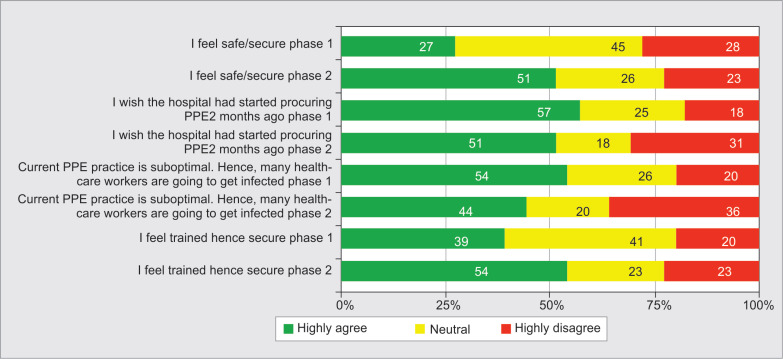
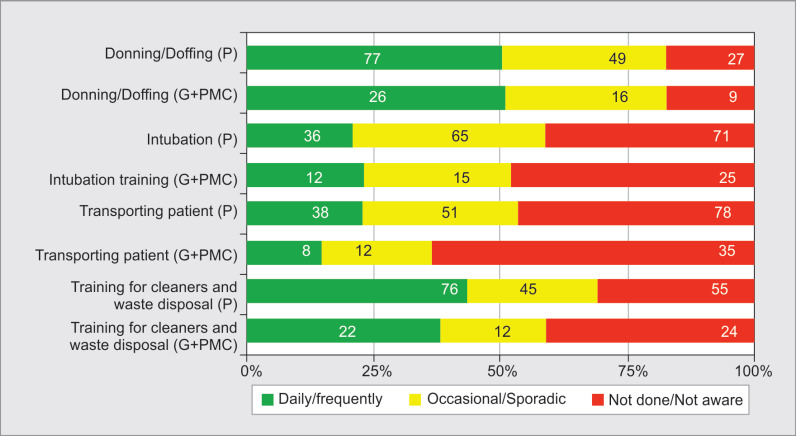
Results: Response rate was 25% from 22 states. PPE practice varied between states and between private, government, and medical colleges. Between phase 1 and phase 2, all aspects of PPE training improved: donning/doffing 43% vs 66%, respectively; p value <0.01); safe waste disposal practices (38% vs 52%; p value = 0.09); intubation training (18% vs 31%; p value = 0.05); and transport (18% vs 31%; p value = 0.05). Perception of confidence for adequate PPE-training improved from 39 to 53% (p value = 0.26). In all, 47 to 60% ICUs adhered to MoH recommendations. Wearing N95-masks at all times increased from 47 to 60% (p value = 0.89). Very few ICUs provided quantitative/qualitative N95 masks fit testing (12% vs 29%; p value <0.01). Low-cost practices like "buddy-system" for donning-doffing (27% vs 44%; p value = 0.02) and showering after PPE breach (10% vs 8%; p value = 0.63) were underutilized. There was reluctance to PPE reuse. In all, 71% were unaware/diffident about PPE inventory.
Conclusion: Despite interstate variability, most ICUs conformed to MoH recommendations. This survey conducted during initial pandemic phase demonstrated improved PPE preparedness uniformly across India with scope for further improvement. We suggest implementation of quality improvement measures to improve pandemic preparedness and minimize HCW infection rates, focused on regular PPE training, buddy system, and PPE-breach management.
How to cite this article: Haji JY, Subramaniam A, Kumar P, Ramanathan K, Rajamani A. State of Personal Protective Equipment Practice in Indian Intensive Care Units amidst COVID-19 Pandemic: A Nationwide Survey. Indian J Crit Care Med 2020;24(9):809-816.
Keywords: COVID-19; Donning-doffing; HCW infections; Healthcare workers; Personal protective equipment preparedness; Personal protective equipment training; SARS-CoV-2.
Copyright © 2020; Jaypee Brothers Medical Publishers (P) Ltd.
Conflict of interest statement
Source of support: Nil Conflict of interest: None
Figures
References
-
- S D. 10 per cent cases linked to hospital infections in Mumbai, point to lack of stringent protocols. Times of India 2020 April 10th 2020.
-
- Ong SWX, Tan YK, Chia PY, Lee TH, Ng OT, Wong MSY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323(16):1610–1612. doi: 10.1001/jama.2020.3227. DOI: - DOI - PMC - PubMed
-
- Rajamani A, Subramaniam A, Shekar K, Haji J, Luo J, Bihari S, et al. Variations in personal protective equipment preparedness in intensive care units during the COVID-19 pandemic: a survey of Asia-pacific countries. medRxiv. 2020;2020
LinkOut - more resources
Full Text Sources
Miscellaneous