

AQP4-IgG and MOG-IgG Related Optic Neuritis-Prevalence, Optical Coherence Tomography Findings, and Visual Outcomes: A Systematic Review and Meta-Analysis
- PMID: 33132999
- PMCID: PMC7578376
- DOI: 10.3389/fneur.2020.540156
AQP4-IgG and MOG-IgG Related Optic Neuritis-Prevalence, Optical Coherence Tomography Findings, and Visual Outcomes: A Systematic Review and Meta-Analysis
Abstract
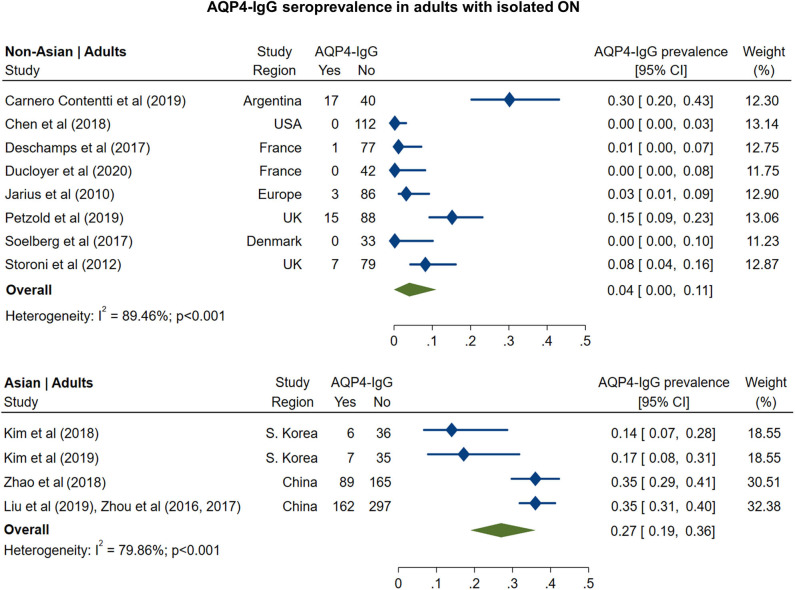
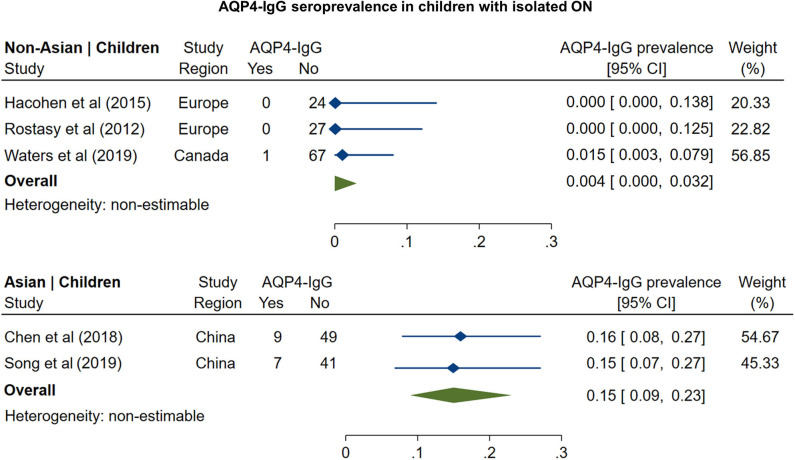
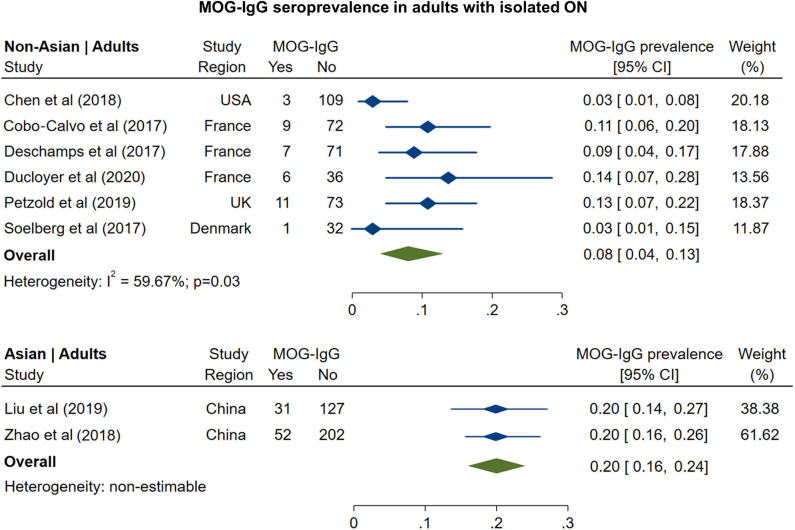
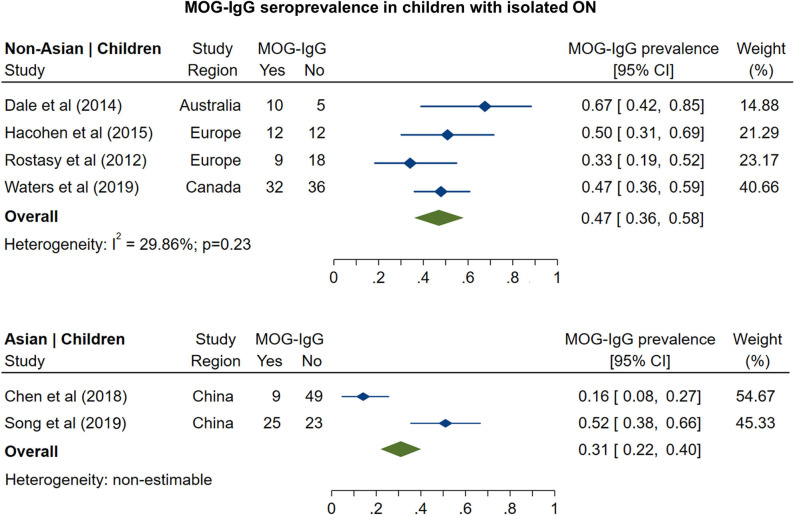
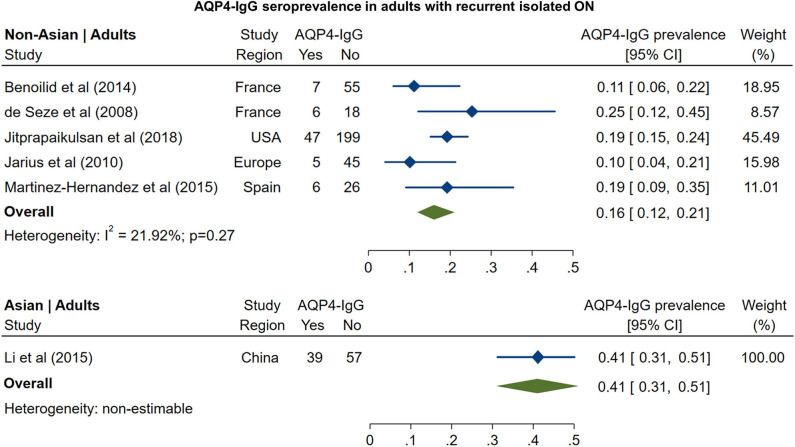
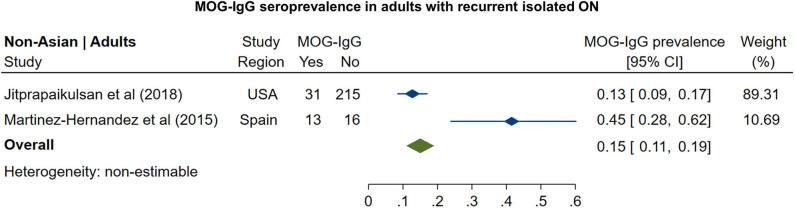
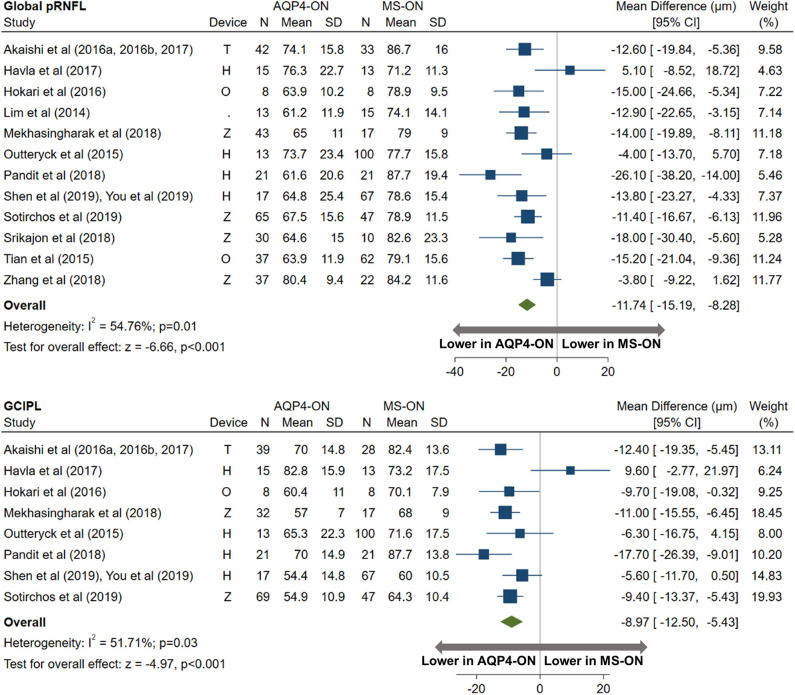
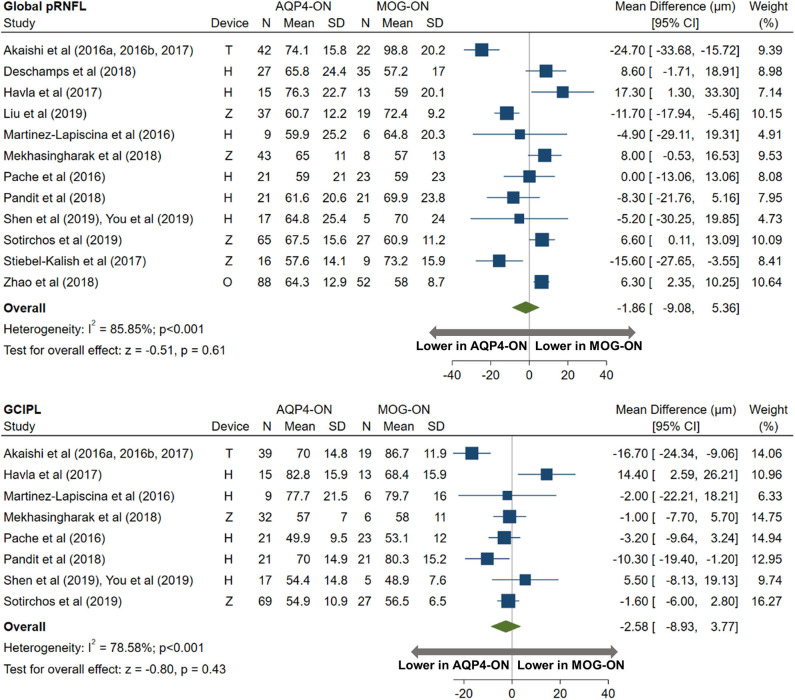
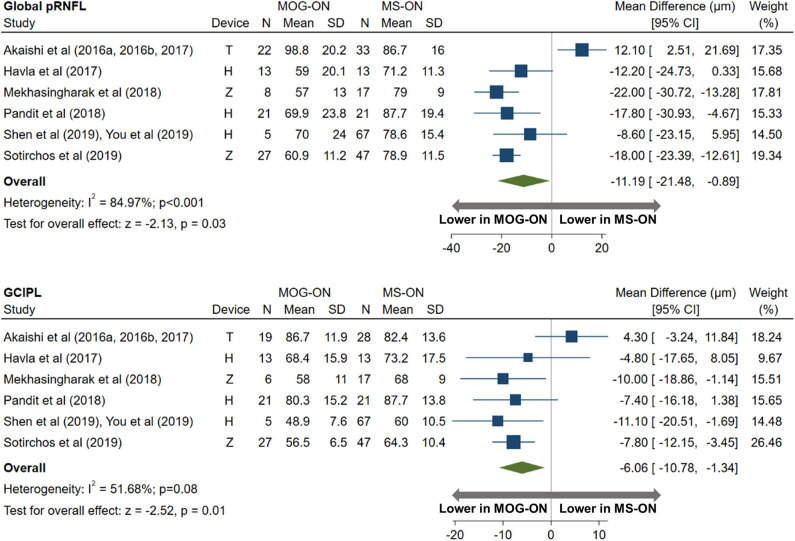
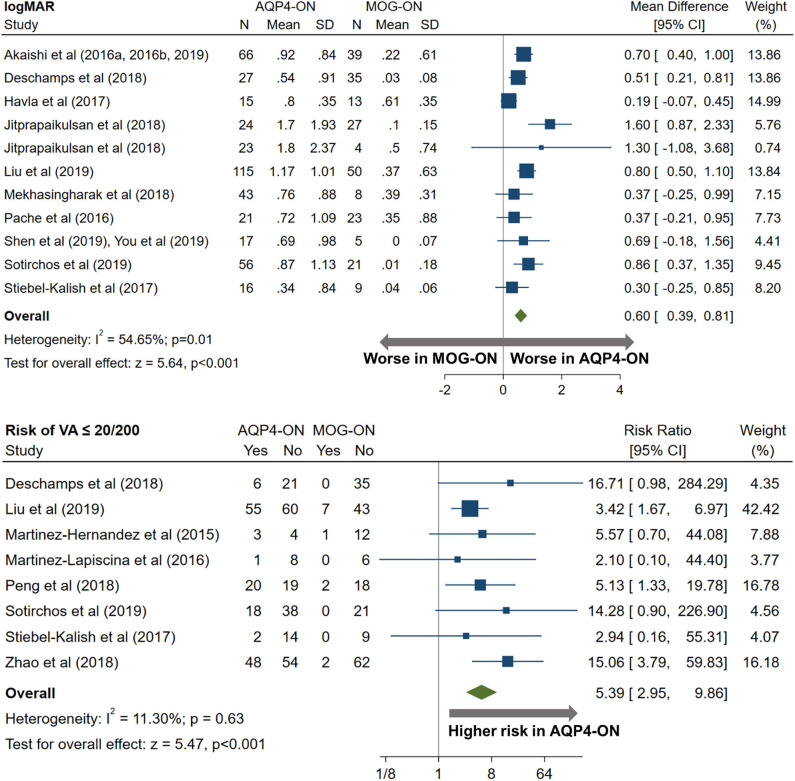
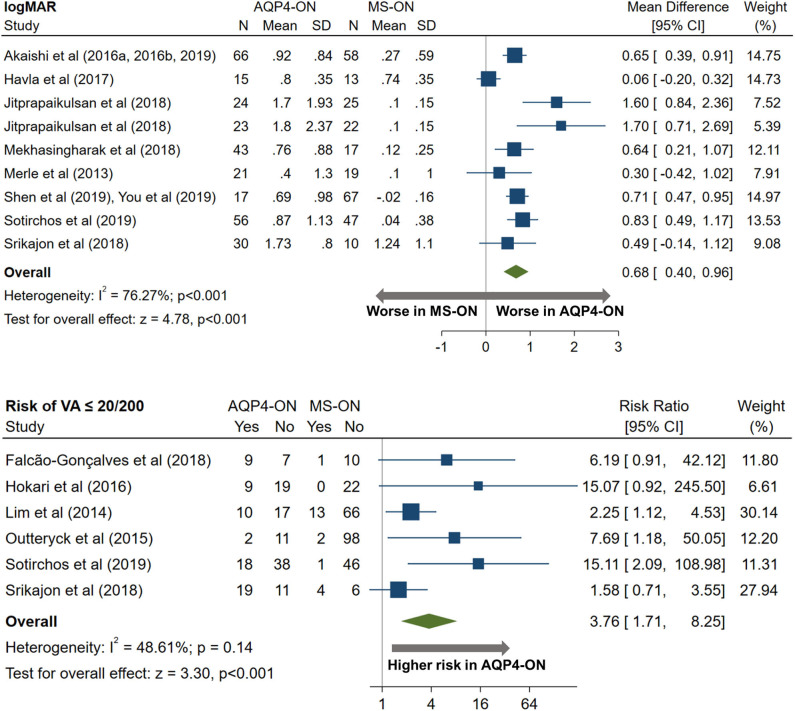
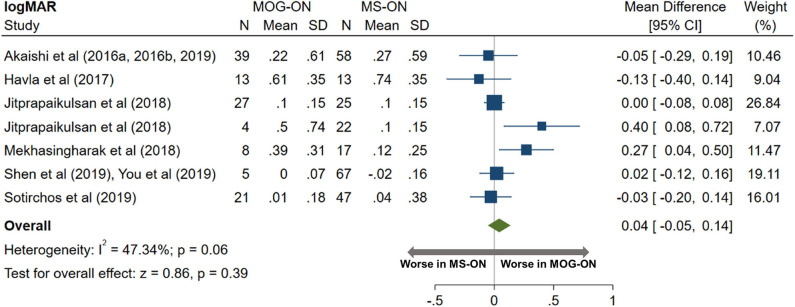
Background: Optic neuritis (ON) is a cardinal manifestation of multiple sclerosis (MS), aquaporin-4 (AQP4)-IgG-, and myelin oligodendrocyte glycoprotein (MOG)-IgG-associated disease. However, the prevalence of AQP4-IgG seropositivity and MOG-IgG seropositivity in isolated ON is unclear, and studies comparing visual outcomes and optical coherence tomography (OCT)-derived structural retinal measures between MS-ON, AQP4-ON, and MOG-ON eyes are limited by small sample sizes. Objectives: (1) To assess the prevalence of AQP4-IgG and MOG-IgG seropositivity among patients presenting with isolated ON; (2) to compare visual outcomes and OCT measures between AQP4-ON, MOG-ON, and MS-ON eyes. Methods: In this systematic review and meta-analysis, a total of 65 eligible studies were identified by PubMed search. Statistical analyses were performed with random effects models. Results: In adults with isolated ON, AQP4-IgG seroprevalence was 4% in non-Asian and 27% in Asian populations, whereas MOG-IgG seroprevalence was 8 and 20%, respectively. In children, AQP4-IgG seroprevalence was 0.4% in non-Asian and 15% in Asian populations, whereas MOG-IgG seroprevalence was 47 and 31%, respectively. AQP4-ON eyes had lower peri-papillary retinal nerve fiber layer (pRNFL; -11.7 μm, 95% CI: -15.2 to -8.3 μm) and macular ganglion cell + inner plexiform layer (GCIPL; -9.0 μm, 95% CI: -12.5 to -5.4 μm) thicknesses compared with MS-ON eyes. Similarly, pRNFL (-11.2 μm, 95% CI: -21.5 to -0.9 μm) and GCIPL (-6.1 μm, 95% CI: -10.8 to -1.3 μm) thicknesses were lower in MOG-ON compared to MS-ON eyes, but did not differ between AQP4-ON and MOG-ON eyes (pRNFL: -1.9 μm, 95% CI: -9.1 to 5.4 μm; GCIPL: -2.6 μm, 95% CI: -8.9 to 3.8 μm). Visual outcomes were worse in AQP4-ON compared to both MOG-ON (mean logMAR difference: 0.60, 95% CI: 0.39 to 0.81) and MS-ON eyes (mean logMAR difference: 0.68, 95% CI: 0.40 to 0.96) but were similar in MOG-ON and MS-ON eyes (mean logMAR difference: 0.04, 95% CI: -0.05 to 0.14). Conclusions: AQP4-IgG- and MOG-IgG-associated disease are important diagnostic considerations in adults presenting with isolated ON, especially in Asian populations. Furthermore, MOG-IgG seroprevalence is especially high in pediatric isolated ON, in both non-Asian and Asian populations. Despite a similar severity of GCIPL and pRNFL thinning in AQP4-ON and MOG-ON, AQP4-ON is associated with markedly worse visual outcomes.
Keywords: aquaporin-4 (AQP4) IgG; myelin oligodendrocyte glycoprotein (MOG) IgG associated disease; neuromyelitis optica (NMO); neuromyelitis optica spectrum disorder (NMOsd); optic neuritis (ON); optical coherence tomography (OCT); retina; visual acuity.
Copyright © 2020 Filippatou, Mukharesh, Saidha, Calabresi and Sotirchos.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous