

Paying for Performance Improvement in Quality and Outcomes of Cardiovascular Care: Challenges and Prospects
- PMID: 33133359
- PMCID: PMC7587319
- DOI: 10.14797/mdcj-16-3-225
Paying for Performance Improvement in Quality and Outcomes of Cardiovascular Care: Challenges and Prospects
Abstract
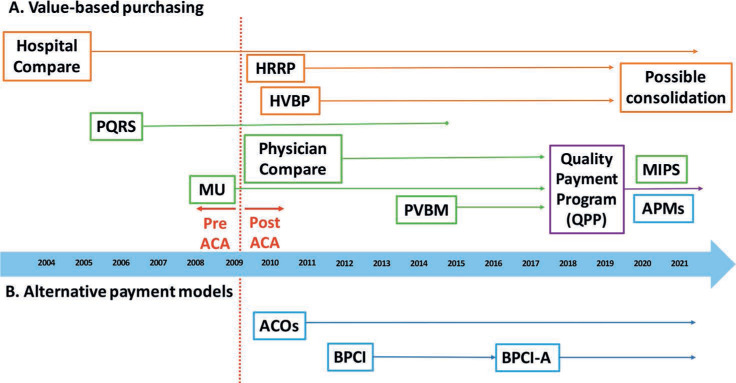
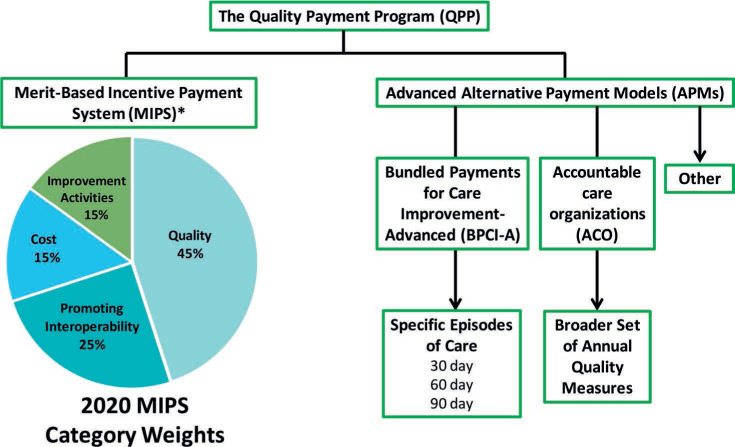
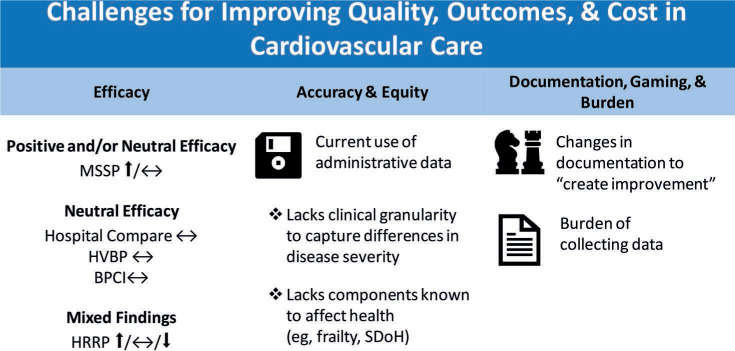
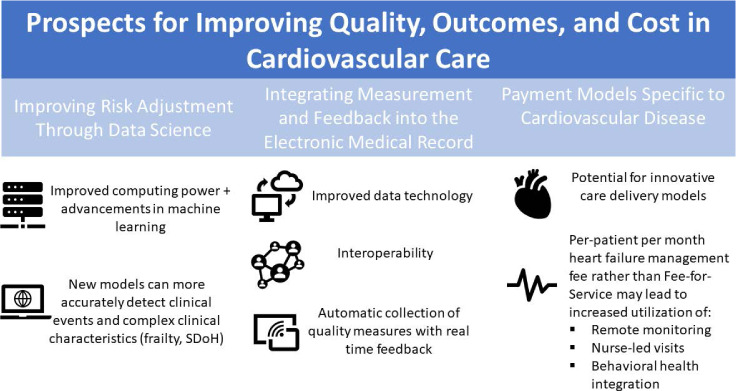
Over the past two decades, Medicare and other payers have been looking at ways to base payment for cardiovascular care on the quality and outcomes of care delivered. Public reporting of hospital performance on a series of quality measures began in 2004 with basic processes of care such as aspirin use and influenza vaccination, and it expanded in later years to include outcomes such as mortality and readmission rates. Following the passage of the Affordable Care Act in March 2010, Medicare and other payers moved forward with pay-for-performance programs, more commonly referred to as value-based purchasing (VBP) programs. These programs are largely based on an underlying fee-for-service payment infrastructure and give hospitals and clinicians bonuses or penalties based on their performance. Another new payment mechanism, called alternative payment models (APMs), aims to move towards episode-based or global payments to improve quality and efficiency. The two most relevant APMs for cardiovascular care include Accountable Care Organizations and bundled payments. Both VBP programs and APMs have challenges related to program efficacy, accuracy, and equity. In fact, despite over a decade of progress in measuring and incentivizing high-quality care delivery within cardiology, major limitations remain. Many of the programs have had little benefit in terms of clinical outcomes yet have led to marked administrative burden for participants. However, there are several encouraging prospects to aid the successful implementation of value-based high-quality cardiovascular care, such as more sophisticated data science to improve risk adjustment and flexible electronic health records to decrease administrative burden. Furthermore, payment models designed specifically for cardiovascular care could incentivize innovative care delivery models that could improve quality and outcomes for patients. This review provides an overview of current efforts, largely at the federal level, to pay for high-quality cardiovascular care and discusses the challenges and prospects related to doing so.
Keywords: alternative payment models; cardiovascular care; pay for performance; value-based purchasing.
© 2020 Houston Methodist Hospital Houston, Texas.
Conflict of interest statement
Conflict of Interest Disclosure: Dr. Joynt Maddox does contract work for the United States Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. There are no other financial conflicts of interest to report.
Figures
Similar articles
-
Value-Based Payment Reforms in Cardiovascular Care: Progress to Date and Next Steps.Methodist Debakey Cardiovasc J. 2020 Jul-Sep;16(3):232-240. doi: 10.14797/mdcj-16-3-232. Methodist Debakey Cardiovasc J. 2020. PMID: 33133360 Free PMC article. Review.
-
Do cardiology quality measures actually improve patient outcomes?J Am Heart Assoc. 2014 Feb 7;3(1):e000404. doi: 10.1161/JAHA.113.000404. J Am Heart Assoc. 2014. PMID: 24510114 Free PMC article. Review. No abstract available.
-
Advancing Value-Based Models for Heart Failure: A Call to Action From the Value in Healthcare Initiative's Value-Based Models Learning Collaborative.Circ Cardiovasc Qual Outcomes. 2020 May;13(5):e006483. doi: 10.1161/CIRCOUTCOMES.120.006483. Epub 2020 May 12. Circ Cardiovasc Qual Outcomes. 2020. PMID: 32393125
-
Current State of Value-Based Purchasing Programs.Circulation. 2016 May 31;133(22):2197-205. doi: 10.1161/CIRCULATIONAHA.115.010268. Circulation. 2016. PMID: 27245648 Free PMC article. Review.
-
Medicare Program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems and Quality Reporting Programs; Organ Procurement Organization Reporting and Communication; Transplant Outcome Measures and Documentation Requirements; Electronic Health Record (EHR) Incentive Programs; Payment to Nonexcepted Off-Campus Provider-Based Department of a Hospital; Hospital Value-Based Purchasing (VBP) Program; Establishment of Payment Rates Under the Medicare Physician Fee Schedule for Nonexcepted Items and Services Furnished by an Off-Campus Provider-Based Department of a Hospital. Final rule with comment period and interim final rule with comment period.Fed Regist. 2016 Nov 14;81(219):79562-892. Fed Regist. 2016. PMID: 27906530
Cited by
-
Quality measurement for cardiovascular diseases and cancer in hospital value-based healthcare: a systematic review of the literature.BMC Health Serv Res. 2022 Aug 1;22(1):979. doi: 10.1186/s12913-022-08347-x. BMC Health Serv Res. 2022. PMID: 35915449 Free PMC article.
-
Effects of the Million Hearts Model on Myocardial Infarctions, Strokes, and Medicare Spending: A Randomized Clinical Trial.JAMA. 2023 Oct 17;330(15):1437-1447. doi: 10.1001/jama.2023.19597. JAMA. 2023. PMID: 37847273 Free PMC article. Clinical Trial.
-
How to Use Costs in Value-Based Healthcare: Learning from Real-life Examples.J Gen Intern Med. 2024 Mar;39(4):683-689. doi: 10.1007/s11606-023-08423-w. Epub 2023 Dec 22. J Gen Intern Med. 2024. PMID: 38135776 Free PMC article.
-
Association Between Increased Hospital Reimbursement for Cardiac Rehabilitation and Utilization of Cardiac Rehabilitation by Medicare Beneficiaries: An Interrupted Time Series.Circ Cardiovasc Qual Outcomes. 2021 Mar;14(3):e006572. doi: 10.1161/CIRCOUTCOMES.120.006572. Epub 2021 Mar 8. Circ Cardiovasc Qual Outcomes. 2021. PMID: 33677975 Free PMC article.
References
-
- Wasfy JH, Borden WB, Secemsky EA, McCabe JM, Yeh RW. Public reporting in cardiovascular medicine: accountability, unintended consequences, and promise for improvement. Circulation. 2015 Apr 28;131(17):1518–27. - PubMed
-
- Zuckerman RB, Sheingold SH, Epstein AM. The Hospital Readmissions Reduction Program. N Engl J Med. 2016 Aug 4;375(5):494. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
