

Defining the advantages and exposing the limitations of endoscopic variceal ligation in controlling acute bleeding and achieving complete variceal eradication
- PMID: 33133373
- PMCID: PMC7579524
- DOI: 10.4253/wjge.v12.i10.365
Defining the advantages and exposing the limitations of endoscopic variceal ligation in controlling acute bleeding and achieving complete variceal eradication
Abstract
Background: Bleeding esophageal varices (BEV) is a potentially life-threatening complication in patients with portal hypertension with mortality rates as high as 25% within six weeks of the index variceal bleed. After control of the initial bleeding episode patients should enter a long-term surveillance program with endoscopic intervention combined with non-selective β-blockers to prevent further bleeding and eradicate EV.
Aim: To assess the efficacy of endoscopic variceal ligation (EVL) in controlling acute variceal bleeding, preventing variceal recurrence and rebleeding and achieving complete eradication of esophageal varices (EV) in patients who present with BEV.
Methods: A prospectively documented single-center database was used to retrospectively identify all patients with BEV who were treated with EVL between 2000 and 2018. Control of acute bleeding, variceal recurrence, rebleeding, eradication and survival were analyzed using Baveno assessment criteria.
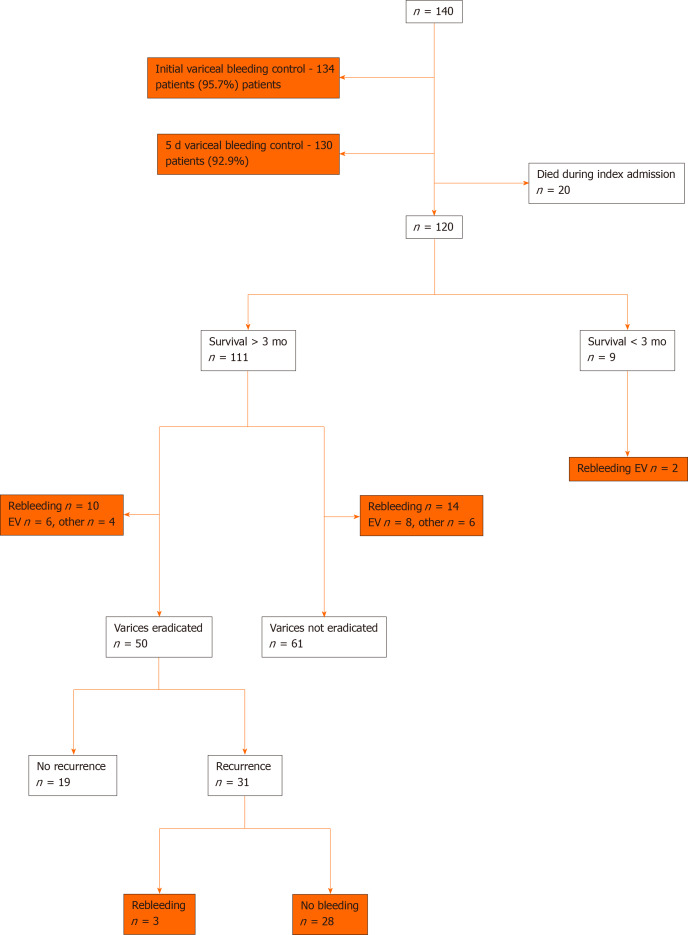
Results: One hundred and forty patients (100 men, 40 women; mean age 50 years; range, 21-84 years; Child-Pugh grade A = 32; B = 48; C = 60) underwent 160 emergency and 298 elective EVL interventions during a total of 928 endoscopy sessions. One hundred and fourteen (81%) of the 140 patients had variceal bleeding that was effectively controlled during the index banding procedure and never bled again from EV, while 26 (19%) patients had complicated and refractory variceal bleeding. EVL controlled the acute sentinel variceal bleed during the first endoscopic intervention in 134 of 140 patients (95.7%). Six patients required balloon tamponade for control and 4 other patients rebled in hospital. Overall 5-d endoscopic failure to control variceal bleeding was 7.1% (n = 10) and four patients required a salvage transjugular intrahepatic portosystemic shunt. Index admission mortality was 14.2% (n = 20). EV were completely eradicated in 50 of 111 patients (45%) who survived > 3 mo of whom 31 recurred and 3 rebled. Sixteen (13.3%) of 120 surviving patients subsequently had 21 EV rebleeding episodes and 10 patients bled from other sources after discharge from hospital. Overall rebleeding from all sources after 2 years was 21.7% (n = 26). Sixty-nine (49.3%) of the 140 patients died, mainly due to liver failure (n = 46) during follow-up. Cumulative survival for the 140 patients was 71.4% at 1 year, 65% at 3 years, 60% at 5 years and 52.1% at 10 years.
Conclusion: EVL was highly effective in controlling the sentinel variceal bleed with an overall 5-day failure to control bleeding of 7.1%. Although repeated EVL achieved complete variceal eradication in less than half of patients with BEV, of whom 62% recurred, there was a significant reduction in subsequent rebleeding.
Keywords: Endoscopy; Esophageal varices; Secondary prophylaxis; Variceal bleeding; Variceal ligation; Variceal recurrence.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Figures
References
-
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65:310–335. - PubMed
-
- Amitrano L, Guardascione MA, Manguso F, Bennato R, Bove A, DeNucci C, Lombardi G, Martino R, Menchise A, Orsini L, Picascia S, Riccio E. The effectiveness of current acute variceal bleed treatments in unselected cirrhotic patients: refining short-term prognosis and risk factors. Am J Gastroenterol. 2012;107:1872–1878. - PubMed
-
- Fortune BE, Garcia-Tsao G, Ciarleglio M, Deng Y, Fallon MB, Sigal S, Chalasani NP, Lim JK, Reuben A, Vargas HE, Abrams G, Lewis MD, Hassanein T, Trotter JF, Sanyal AJ, Beavers KL, Ganger D, Thuluvath PJ, Grace ND, Groszmann RJ Vapreotide Study Group. Child-Turcotte-Pugh Class is Best at Stratifying Risk in Variceal Hemorrhage: Analysis of a US Multicenter Prospective Study. J Clin Gastroenterol. 2017;51:446–453. - PMC - PubMed
-
- Tripathi D, Stanley AJ, Hayes PC, Patch D, Millson C, Mehrzad H, Austin A, Ferguson JW, Olliff SP, Hudson M, Christie JM Clinical Services and Standards Committee of the British Society of Gastroenterology. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64:1680–1704. - PMC - PubMed
-
- de Franchis R Baveno VI Faculty. Expanding consensus in portal hypertension: Report of the Baveno VI Consensus Workshop: Stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63:743–752. - PubMed
LinkOut - more resources
Full Text Sources
