

Total Hip Arthroplasty in the Obese Patient: Tips and Tricks and Review of the Literature
- PMID: 33133400
- PMCID: PMC7572957
- DOI: 10.1007/s43465-020-00164-w
Total Hip Arthroplasty in the Obese Patient: Tips and Tricks and Review of the Literature
Abstract
Aim: There is a lack of consensus on the optimal method of performing primary hip arthroplasty in obese patients and limited evidence. This article presents a series of considerations based on the authors' experiences as well as a review of the literature.
Preoperative care: In the preoperative phase, an informed consent process is recommended. Weight loss is recommended according to NHS England guidelines, and body habitus should be taken into account. When templating, steps are taken to avoid overestimating the implant size.
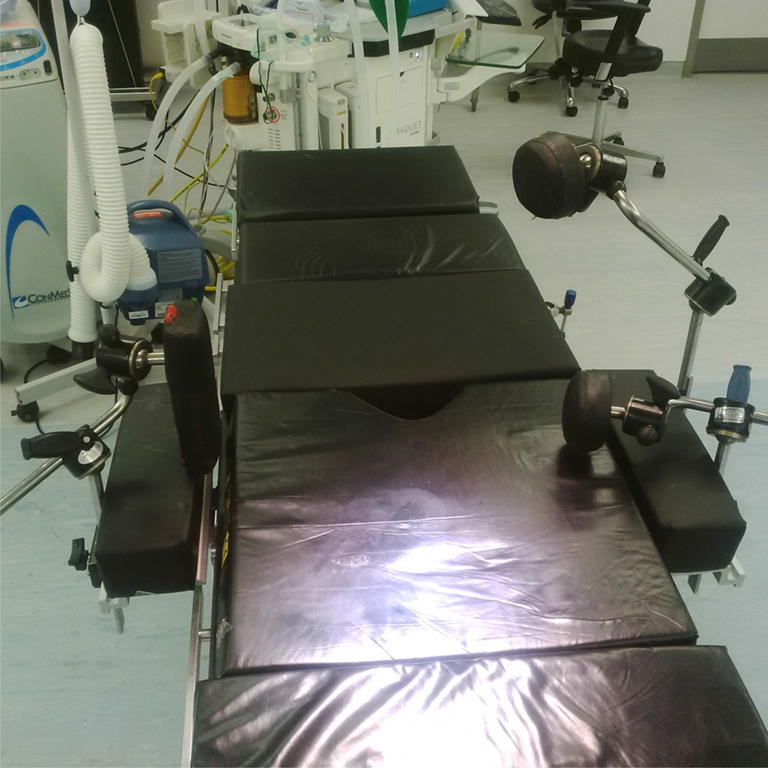
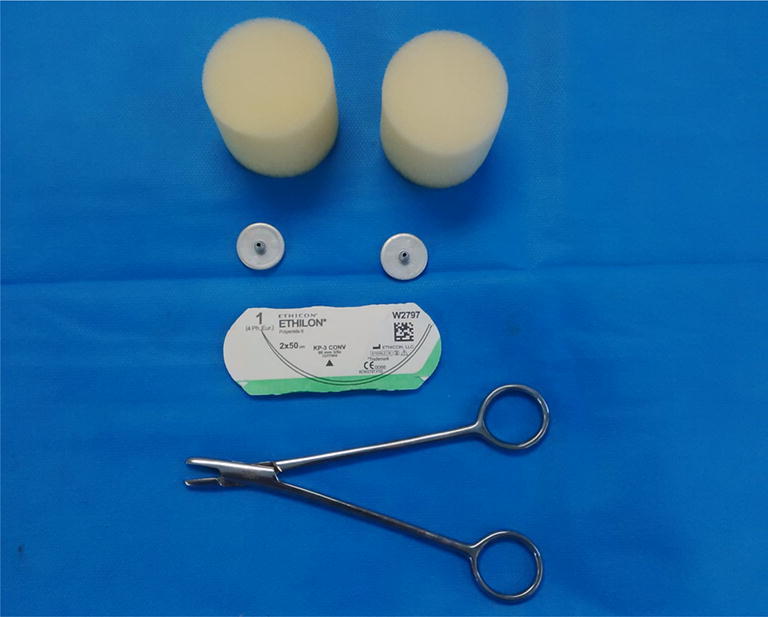
Surgical procedure: During the surgical procedure, specialist bariatric equipment is utilised: bariatric beds, extra supports, hover mattresses, longer scalpels, diathermy, cell saver and minimally invasive surgery equipment. Communication with the anaesthetist and surgical team to anticipate is vital. Intraoperative sizing and imaging, if required, should be considered. Pneumatic foot pumps are preferable for VTE prophylaxis. Regional anaesthesia is preferred due to technical difficulty. IV antibiotics and tranexamic acid are recommended. The anterior and posterior surgical approaches are most frequently used; we advocate posterior. Incisions are extensile and a higher offset is considered intraoperatively, as well as dual mobility and constrained liners to reduce dislocation risk. When closing the wound, Charnely button and sponge should be considered as well as negative pressure wound dressings (iNPWTd) and drains.
Post-operative considerations: Postoperatively, difficult extubation should be anticipated with ITU/HDU beds available. Epidural anaesthetics for postoperative pain management require higher nursing vigilance. Chemical prophylaxis is recommended.
Conclusion: Despite being technically more difficult with higher risks, functional outcomes are comparable with patients with a normal BMI.
Keywords: Hip arthroplasty; Obesity; Technical; Tips tricks; Total hip replacement.
© Indian Orthopaedics Association 2020.
Conflict of interest statement
Conflict of interestAll authors declare that they have no conflict of interest.
Figures

Similar articles
-
Dual-mobility or Constrained Liners Are More Effective Than Preoperative Bariatric Surgery in Prevention of THA Dislocation.Clin Orthop Relat Res. 2016 Oct;474(10):2202-10. doi: 10.1007/s11999-016-4859-3. Clin Orthop Relat Res. 2016. PMID: 27130648 Free PMC article.
-
Dual Mobile Total Hip Replacement in Super Obesity: A Case Report and Review of Literature.J Orthop Case Rep. 2021 Oct;11(10):91-95. doi: 10.13107/jocr.2021.v11.i10.2486. J Orthop Case Rep. 2021. PMID: 35415086 Free PMC article.
-
[Local Application of Tranexamic Acid in Total Hip Arthroplasty Decreases Blood Loss and Consumption of Blood Transfusion].Acta Chir Orthop Traumatol Cech. 2017;84(4):254-262. Acta Chir Orthop Traumatol Cech. 2017. PMID: 28933328 Czech.
-
Effect of non-surgical, non-pharmacological weight loss interventions in patients who are obese prior to hip and knee arthroplasty surgery: a rapid review.Syst Rev. 2015 Sep 27;4:121. doi: 10.1186/s13643-015-0107-2. Syst Rev. 2015. PMID: 26410227 Free PMC article. Review.
-
[The perioperative phase as a part of anesthesia. Tasks of the recovery room].Anaesthesist. 1997 Oct;46 Suppl 2:S109-13. doi: 10.1007/pl00002470. Anaesthesist. 1997. PMID: 9432872 Review. German.
Cited by
-
Increased patient body mass index is associated with increased surgeon physiologic stress during total hip arthroplasty.Arch Orthop Trauma Surg. 2024 May;144(5):2357-2363. doi: 10.1007/s00402-024-05251-3. Epub 2024 Mar 18. Arch Orthop Trauma Surg. 2024. PMID: 38498157
-
Orthopaedic Nurse Navigators and Total Joint Arthroplasty Preoperative Optimization: Obesity and Malnutrition-Part Four of the Movement Is Life Special ONJ Series.Orthop Nurs. 2024 Mar-Apr 01;43(2):75-83. doi: 10.1097/NOR.0000000000001013. Orthop Nurs. 2024. PMID: 38546679 Free PMC article. Review.
-
Is the Direct Anterior Approach for Total Hip Arthroplasty Effective in Obese Patients? Early Clinical and Radiographic Results from a Retrospective Comparative Study.Medicina (Kaunas). 2023 Apr 16;59(4):769. doi: 10.3390/medicina59040769. Medicina (Kaunas). 2023. PMID: 37109727 Free PMC article.
-
[Perioperative management of obese patients undergoing elective hip and knee arthroplasty].Orthopadie (Heidelb). 2025 Feb;54(2):135-143. doi: 10.1007/s00132-024-04597-1. Epub 2025 Jan 20. Orthopadie (Heidelb). 2025. PMID: 39833315 German.
-
A low dislocation rate after revision total hip arthroplasty performed through the anterior approach.Arthroplasty. 2023 Jan 5;5(1):4. doi: 10.1186/s42836-022-00159-y. Arthroplasty. 2023. PMID: 36600292 Free PMC article.
References
-
- NHS Health Survey England,” 2017. [Online]. Retrived from https://digital.nhs.uk/data-and-information/publications/statistical/hea....
-
- H. Q. I. Partnership, “16th Annual Report National Joint Registry for England, Wales, Northern Ireland and the Isle of Man,” 2019.
-
- Culliford D, Maskell J, Judge A, Cooper C, Prieto-Alhambra D, Arden N. Future projections of total hip and knee arthroplasty in the UK: Results from the UK Clinical Practice Research Datalink. Osteoarthritis and Cartlidge Journal. 2015;23:594–600. - PubMed
-
- Changulani M, Kalairajah Y, Peel T, Field R. The relationship between obesity and the age at which hip and knee replacement is undertaken. J Bone Joint Surg. 2008;90:360–363. - PubMed
-
- Malinzak R, Ritter M, Berend M. Morbidly obese, diabetic, younger, and unilateral joint arthroplasty patients have elevated total joint arthroplasty infection rates. The Journal of arthroplasty. 2009;24(6):84–88. - PubMed
Publication types
LinkOut - more resources
Full Text Sources