

Assessment of serum macrophage migration inhibitory factor (MIF), adiponectin, and other adipokines as potential markers of proteinuria and renal dysfunction in lupus nephritis: a cross-sectional study
- PMID: 33133605
- PMCID: PMC7594329
- DOI: 10.1186/s40364-020-00236-x
Assessment of serum macrophage migration inhibitory factor (MIF), adiponectin, and other adipokines as potential markers of proteinuria and renal dysfunction in lupus nephritis: a cross-sectional study
Abstract
Background: To date, the association of serum macrophage migration inhibitory factor (MIF) and serum adipokines with lupus nephritis is controversial.
Objective: To assess the utility of serum MIF, leptin, adiponectin and resistin levels as markers of proteinuria and renal dysfunction in lupus nephritis.
Methods: Cross-sectional study including 196 systemic lupus erythematosus (SLE) patients and 52 healthy controls (HCs). Disease activity was assessed by Systemic Lupus Erythematosus Disease Activity Index (SLEDAI). Renal SLE involvement was investigated by renal-SLEDAI. MIF, adiponectin, leptin and resistin levels were quantified by ELISA. We assessed the correlations of quantitative variables by Spearman correlation (rs). Multivariable linear regression adjusted the variables associated with the severity of proteinuria.
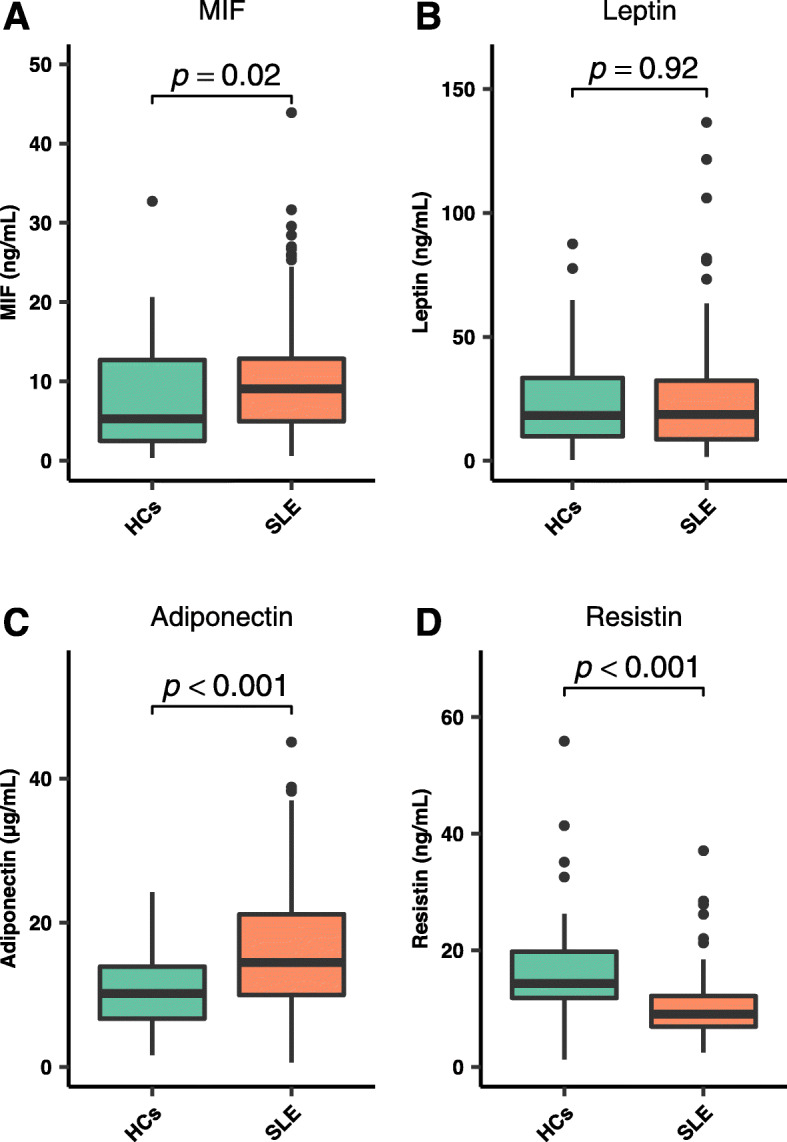
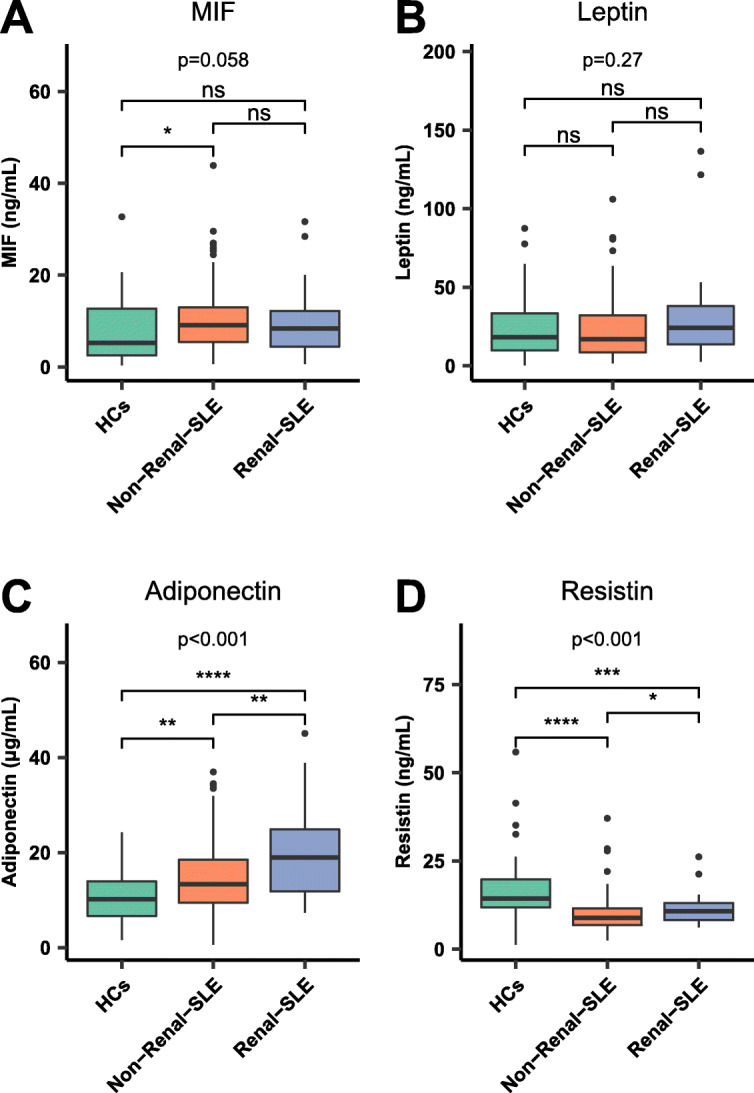
Results: SLE patients had higher MIF (p = 0.02) and adiponectin (p < 0.001) than HCs. Patients with renal SLE involvement (n = 43) had higher adiponectin (19.0 vs 13.3 μg/mL, p = 0.002) and resistin (10.7 vs 8.9 ng/mL, p = 0.01) than patients with non-renal SLE (n = 153). Proteinuria correlated with high adiponectin (r s = 0.19, p < 0.009) and resistin (r s = 0.26, p < 0.001). MIF (r s = 0.27, p = 0.04). Resistin correlated with increased creatinine (r s = 0.18, p = 0.02). High renal-SLEDAI correlated with adiponectin (r s = 0.21, p = 0.004). Multiple linear regression showed that elevated adiponectin (p = 0.02), younger age (p = 0.04) and low MIF (p = 0.02) were associated with the severity of proteinuria. Low MIF and high adiponectin levels interacted to explain the association with the severity of proteinuria (R2 = 0.41).
Conclusions: High adiponectin combined with low MIF concentrations int+eract to explain the severity of proteinuria in renal SLE. These findings highlight the relevance of adiponectin, resistin and MIF as markers of LN.
Keywords: Adipokines; Adiponectin; Biomarkers; Lupus Erythematosus systemic; Lupus nephritis; MIF.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsAll the authors declare that there are no conflicts of interest to disclose.
Figures
References
-
- Plantinga L, Lim SS, Patzer R, McClellan W, Kramer M, Klein M, et al. Incidence of end-stage renal disease among newly diagnosed systemic lupus Erythematosus patients: the Georgia lupus registry: ESRD incidence in SLE patients. Arthritis Care Res. 2016;68:357–365. doi: 10.1002/acr.22685. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
