

A Case of Laryngeal Tuberculosis, Endobronchial Tuberculosis and Pulmonary Tuberculosis Coexistent in an Immunocompetent Host
- PMID: 33133876
- PMCID: PMC7594666
- DOI: 10.7759/cureus.10713
A Case of Laryngeal Tuberculosis, Endobronchial Tuberculosis and Pulmonary Tuberculosis Coexistent in an Immunocompetent Host
Abstract
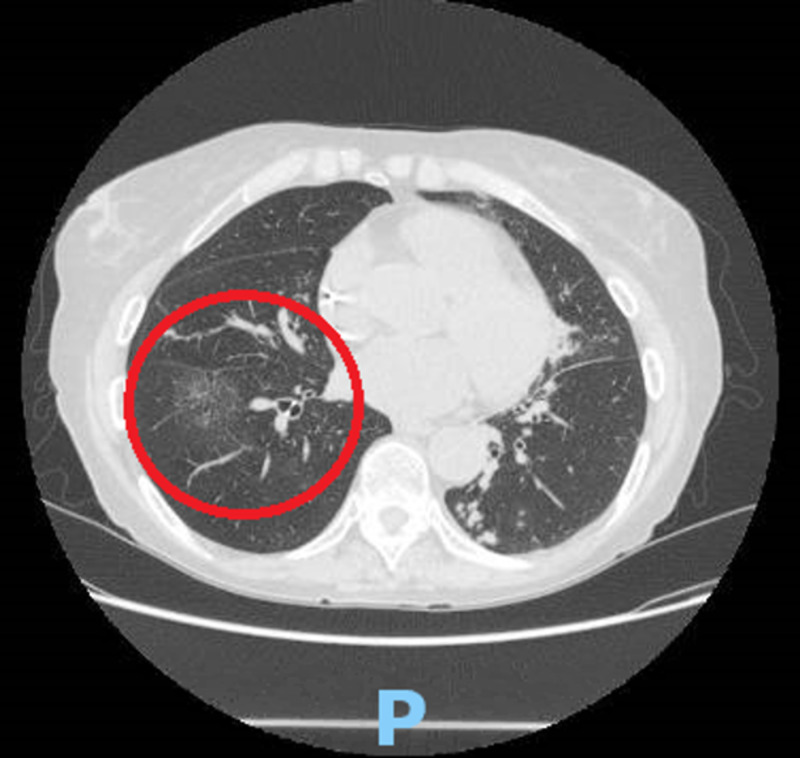
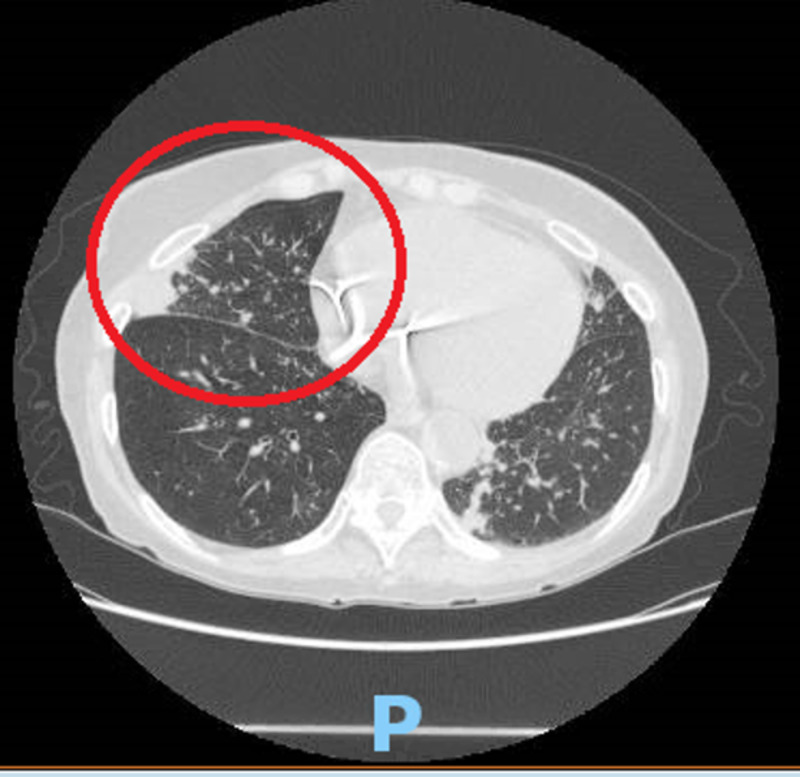
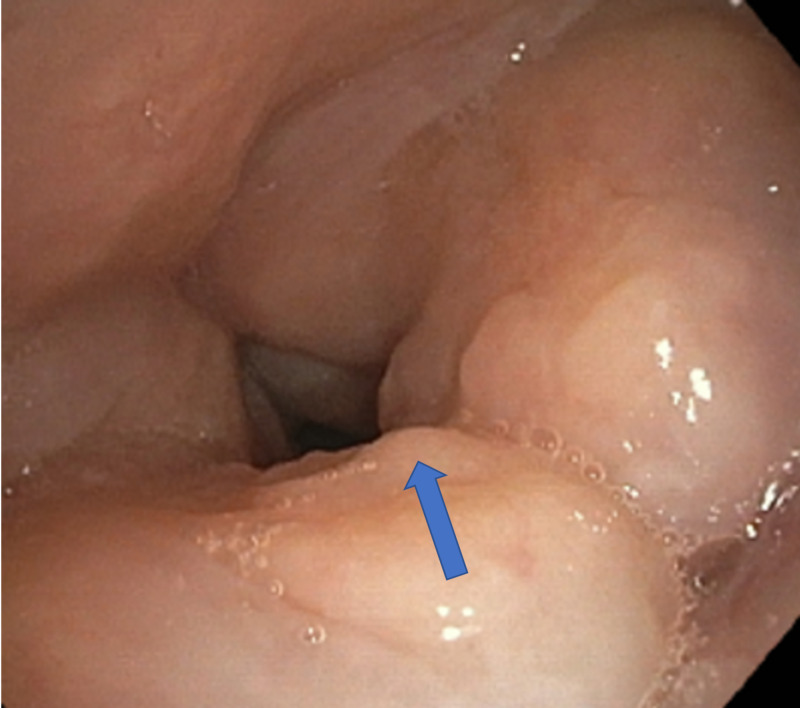
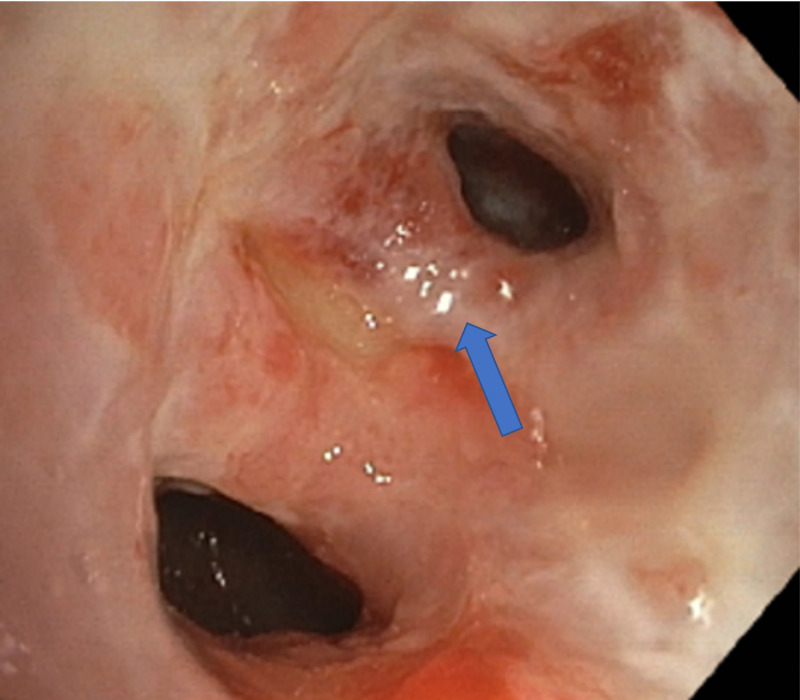
Historically associated with poor prognosis seen in advanced disease, laryngeal tuberculosis (LTB) now represents only 1% of all cases of tuberculosis (TB). The incidence of LTB has decreased drastically with the introduction of anti-tubercular drugs. LTB can be primary or secondary to pulmonary tuberculosis. LTB can mimic laryngeal cancer. We present a case of primary laryngeal TB with descending tracheobronchial spread in an immunocompetent 71-year-old female who developed progressive dysphonia over several months with unintentional weight loss and non-productive cough. Non-contrast enhanced computed tomography (CT) revealed clustering of subcentimeter stellate nodules in the right upper lung field with an enlarging ground-glass opacity in the right lower lung but did not show structural abnormalities within the neck. Positron emission tomography (PET) showed pathologic fluorodeoxyglucose (FDG) uptake within the larynx and trachea with extension into the left mainstream bronchus as well as the proximal left upper and lower lobe bronchi. Diffuse standardized uptake value (SUV) was greatest in the larynx (20.5). Polymerase chain reaction (PCR) on bronchoscope sputum specimen confirmed Mycobacterium tuberculosis. Findings were consistent with primary laryngeal TB with endobronchial extension. She was started on a four-drug regimen comprising of isoniazid, rifampin, ethambutol, and pyrazinamide with a good response. Her close contacts were treated as well. This case highlights the unusual spread of primary laryngeal TB in an immunocompetent host. Early diagnosis can limit adverse complications and unnecessary exposure to healthcare workers. To our knowledge, this is the first case of primary LTB with proximal spread to the tracheobronchial and pulmonary tuberculosis.
Keywords: endobronchial tuberculosis; laryngeal tuberculosis; tuberculosis.
Copyright © 2020, Avula et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Catastrophic Hemoptysis in Concurrent Laryngeal and Endobronchial Tuberculosis in an Immunocompetent Host: Survival Following Brief ECMO Support.Respirol Case Rep. 2025 Jun 18;13(6):e70244. doi: 10.1002/rcr2.70244. eCollection 2025 Jun. Respirol Case Rep. 2025. PMID: 40535727 Free PMC article.
-
Factors Associated with Clinical and Topographical Features of Laryngeal Tuberculosis.PLoS One. 2016 Apr 14;11(4):e0153450. doi: 10.1371/journal.pone.0153450. eCollection 2016. PLoS One. 2016. PMID: 27077734 Free PMC article.
-
API TB Consensus Guidelines 2006: Management of pulmonary tuberculosis, extra-pulmonary tuberculosis and tuberculosis in special situations.J Assoc Physicians India. 2006 Mar;54:219-34. J Assoc Physicians India. 2006. PMID: 16800350
-
[Agranulocytosis due to anti-tuberculosis drugs including isoniazid (INH) and rifampicin (RFP)--a report of four cases and review of the literature].Kekkaku. 2003 Nov;78(11):683-9. Kekkaku. 2003. PMID: 14672045 Review. Japanese.
-
Laryngeal tubercolosis: a case report with focus on voice assessment and review of the literature.Acta Otorhinolaryngol Ital. 2022 Oct;42(5):407-414. doi: 10.14639/0392-100X-N2091. Acta Otorhinolaryngol Ital. 2022. PMID: 36541378 Free PMC article. Review.
References
-
- Coexistence of tuberculosis and malignancy: a mere coincidence or a causal association. Pujani M, Jairajpuri ZS, Khan S, Hassan MJ, Jetley S, Rana S. Trop Doct. 2017;47:101–104. - PubMed
-
- Laryngeal involvement in patients with active pulmonary tuberculosis. Topak M, Oysu C, Yelken K, Sahin-Yilmaz A, Kulekci M. Eur Arch Otorhinolaryngol. 2008;265:327–330. - PubMed
-
- Laryngeal tuberculosis: an often forgotten diagnosis. Rizzo PB, Da Mosto MC, Clari M, Scotton PG, Vaglia A, Marchiori C. Int J Infect Dis. 2003;7:129–131. - PubMed
-
- Epiglottic tuberculosis: differential diagnosis and treatment: case report and review of the literature. Richter B, Fradis M, Köhler G, Ridder GJ. Ann Otol Rhinol Laryngol. 2001;110:197–201. - PubMed
-
- Changing trends in clinical manifestations of laryngeal tuberculosis. Shin JE, Nam SY, Yoo SJ, Kim SY. Laryngoscope. 2000;110:1950–1953. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources