

Toxic Shock Syndrome after Surgery: Case Presentation and Systematic Review of the Literature
- PMID: 33133879
- PMCID: PMC7572075
- DOI: 10.1097/GOX.0000000000002499
Toxic Shock Syndrome after Surgery: Case Presentation and Systematic Review of the Literature
Abstract
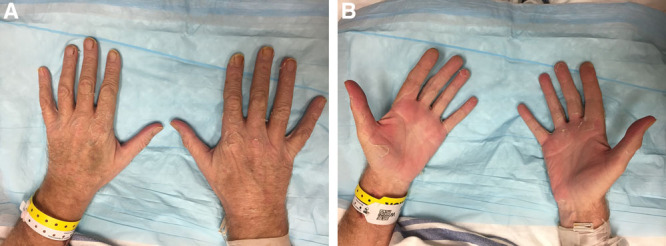
Toxic shock syndrome (TSS) is an underrecognized but highly fatal cause of septic shock in postoperative patients. Although it may present with no overt source of infection, its course is devastating and rapidly progressive. Surgeon awareness is needed to recognize and treat this condition appropriately. In this paper, we aim to describe a case of postoperative TSS, present a systematic review of the literature, and provide an overview of the disease for the surgeon.
Methods: A systematic review of the literature between 1978 and 2018 was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines using the keywords "toxic shock syndrome" and "surgery." Variables of interest were collected in each report.
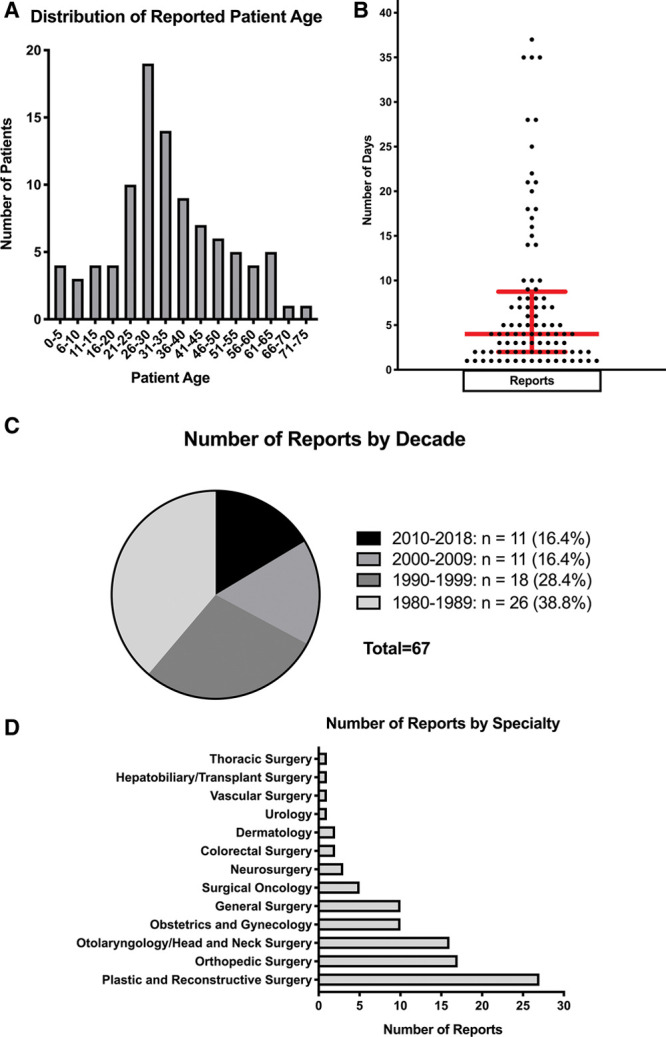
Results: A total of 298 reports were screened, and 67 reports describing 96 individual patients met inclusion criteria. Six reports described a streptococcal cause, although the vast majority attributed TSS to Staphylococcus aureus (SA). The mortality in our review was 9.4%, although 24% of patients suffered some manner of permanent complication. TSS presented at a median of 4 days postoperatively, with most cases occurring within 10 days.
Conclusions: Surgeons must maintain a high index of suspicion for postoperative TSS. Our review demonstrates that TSS should not be excluded despite young patient age, patient health, or relative simplicity of a procedure. Symptoms such as fever, rash, pain out of proportion to examination, and diarrhea or emesis should raise concern for TSS and prompt exploration and cultures even of benign-appearing postoperative wounds.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures

References
-
- Wheeler AP, Bernard GR.Treating patients with severe sepsis. N Engl J Med. 2008;340:207–214. - PubMed
-
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2009;348:1546–1554. - PubMed
-
- Todd J, Fishaut M, Kapral F, et al. Toxic-shock syndrome associated with phage-group-i staphylococci. Lancet. 1978;2:1116–1118. - PubMed
-
- Lappin E, Ferguson AJ.Gram-positive toxic shock syndromes. Lancet Infect Dis. 2009;9:281–290. - PubMed
-
- Gaventa S, Reingold AL, Hightower AW, et al. Active surveillance for toxic shock syndrome in the United States, 1986. Rev Infect Dis. 1989;11suppl 1S28–S34. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous