

New Simple Technique for Syndactyly Release
- PMID: 33133902
- PMCID: PMC7572197
- DOI: 10.1097/GOX.0000000000002842
New Simple Technique for Syndactyly Release
Abstract
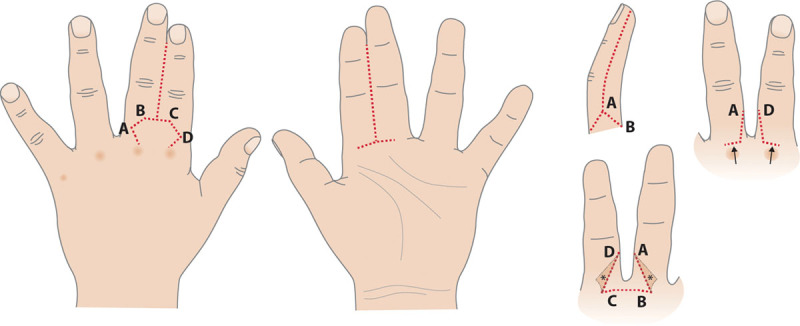
Can good functional and cosmetic result be achieved in syndactyly separation using a straight midline incision with a hexagonal dorsal skin flap?
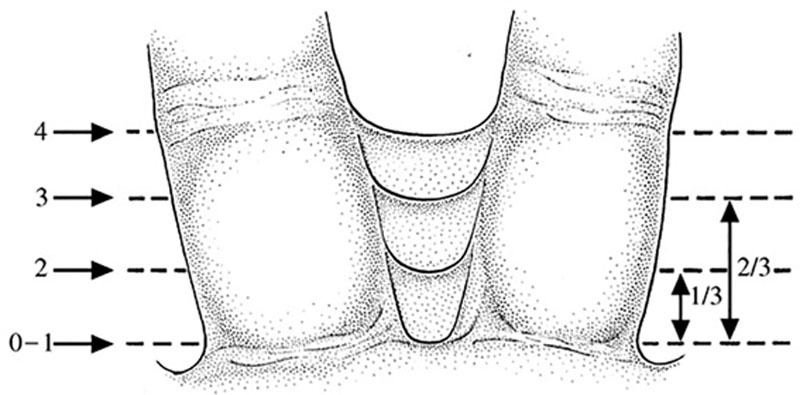
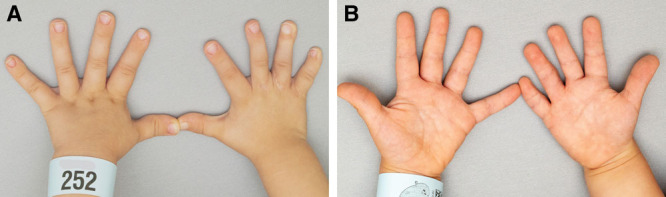
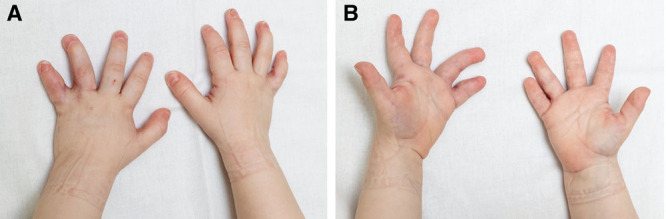
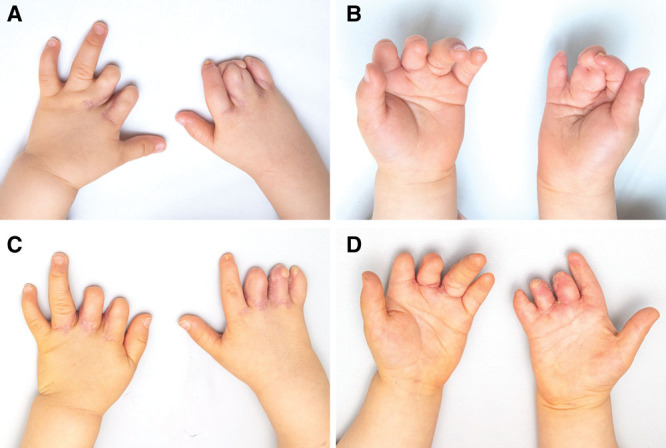
Methods: We performed 39 web reconstructions at a median of 20 months of age (11-43 months) to 26 consecutive children (21 male) with 30 simple, 4 complex, and 5 complicated syndactylies. Eighteen of the simple syndactylies were incomplete, ending at the proximal interphalangeal joint in 15 and at the distal interphalangeal joint in 3. Inguinal skin grafts were used in 2 children with either complex or complicated syndactyly. Operation time was recorded. Complications were registered. Height of the new web spaces was calculated. Parents' satisfaction on both functional and cosmetic outcome was assessed using a Visual Analog Scale from 0 to 100.
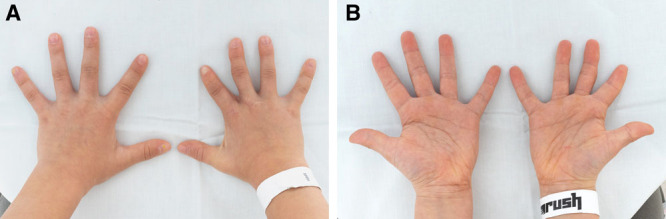
Results: Duration of one web reconstruction ranged from 50 to 95 minutes in simple incomplete, 56 to 135 in simple complete, 116 to 151 in complex, and 72 to 123 in complicated syndactylies. One child had a self-induced bilateral postoperative infection that lead to web creep. Two patients developed hypertrophic scars, which responded well to silicone treatment. Mean cosmetic and functional Visual Analog Scale scores were 87 (45-100) and 92 (63-100), respectively, at a mean follow-up of 1.3 years (range, 0.5-3.7).
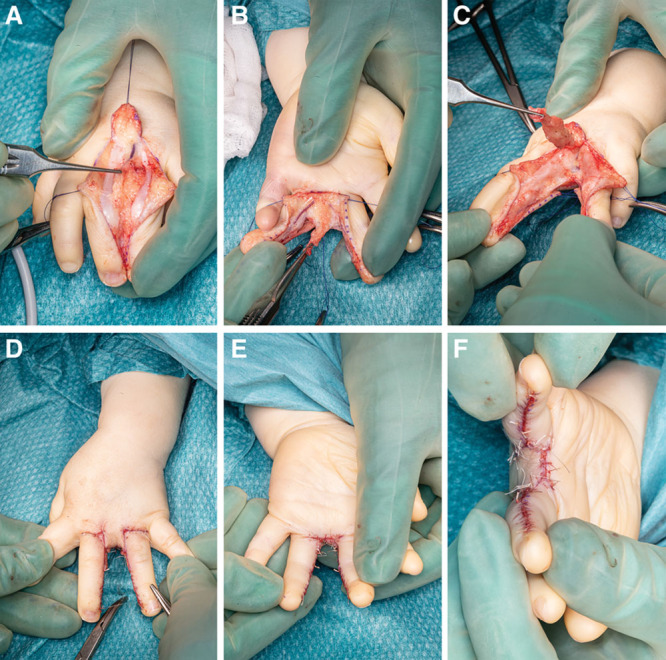
Conclusion: Web reconstruction using a hexagonal dorsal skin flap and straight midline incisions with closure at mid-lateral lines is safe, with good cosmetic and functional outcome in our short-term follow-up.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures
Similar articles
-
Dorsal plane-shaped advancement flap for the reconstruction of web space in syndactyly without skin grafting: A preliminary report.J Plast Reconstr Aesthet Surg. 2015 Nov;68(11):e167-73. doi: 10.1016/j.bjps.2015.06.016. Epub 2015 Jun 27. J Plast Reconstr Aesthet Surg. 2015. PMID: 26190763
-
Interdigitating Rectangular Flaps and Dorsal Pentagonal Island Flap for Syndactyly Release.J Hand Surg Am. 2019 Apr;44(4):288-295. doi: 10.1016/j.jhsa.2019.01.017. J Hand Surg Am. 2019. PMID: 30947823
-
A modification of the Chinese island flap technique for simple incomplete syndactyly release.J Hand Surg Eur Vol. 2009 Feb;34(1):99-103. doi: 10.1177/1753193408094708. Epub 2008 Dec 17. J Hand Surg Eur Vol. 2009. PMID: 19091737
-
The use of a dorsal double-wing flap without skin grafts for congenital syndactyly treatment: A STROBE compliant study.Medicine (Baltimore). 2017 Jul;96(30):e7639. doi: 10.1097/MD.0000000000007639. Medicine (Baltimore). 2017. PMID: 28746226 Free PMC article.
-
Syndactyly Release.Semin Plast Surg. 2016 Nov;30(4):162-170. doi: 10.1055/s-0036-1593478. Semin Plast Surg. 2016. PMID: 27895538 Free PMC article. Review.
Cited by
-
A new concept of webspace reconstruction in syndactyly - An easily reproducible cross-shaped advancement flap.J Hand Microsurg. 2024 May 10;16(4):100081. doi: 10.1016/j.jham.2024.100081. eCollection 2024 Oct. J Hand Microsurg. 2024. PMID: 39234379 Free PMC article.
References
-
- Dao KD, Shin AY, Billings A, et al. Surgical treatment of congenital syndactyly of the hand. J Am Acad Orthop Surg. 2004;12:39–48. - PubMed
-
- Kozin SH, Zlotolow DA.Common pediatric congenital conditions of the hand. Plast Reconstr Surg. 2015;136:241e–257e. - PubMed
-
- Netscher DT, Baumholtz MA.Treatment of congenital upper extremity problems. Plast Reconstr Surg. 2007;119:101e–129e. - PubMed
LinkOut - more resources
Full Text Sources