

Ultrasound-guided Hydro-dissection Facilitates Tissue Expander Placement and Components Separation in Complex Ventral Hernia Repair
- PMID: 33133933
- PMCID: PMC7544377
- DOI: 10.1097/GOX.0000000000003051
Ultrasound-guided Hydro-dissection Facilitates Tissue Expander Placement and Components Separation in Complex Ventral Hernia Repair
Abstract
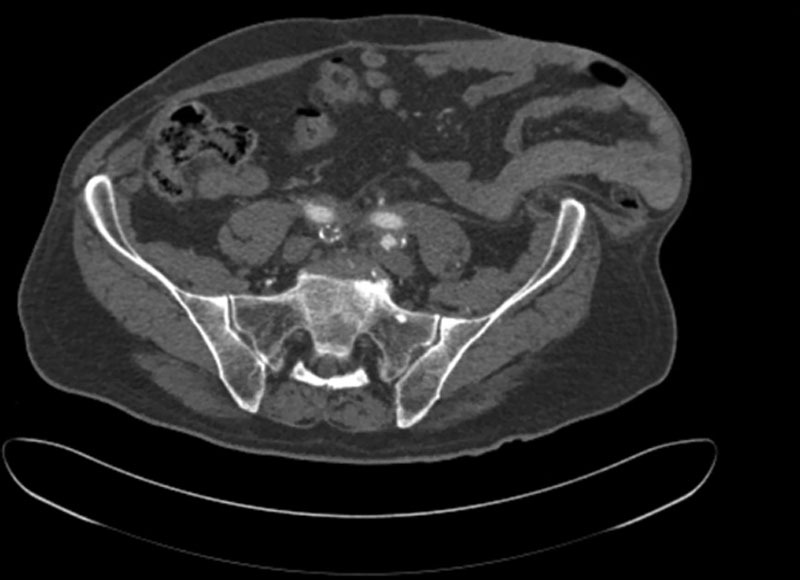
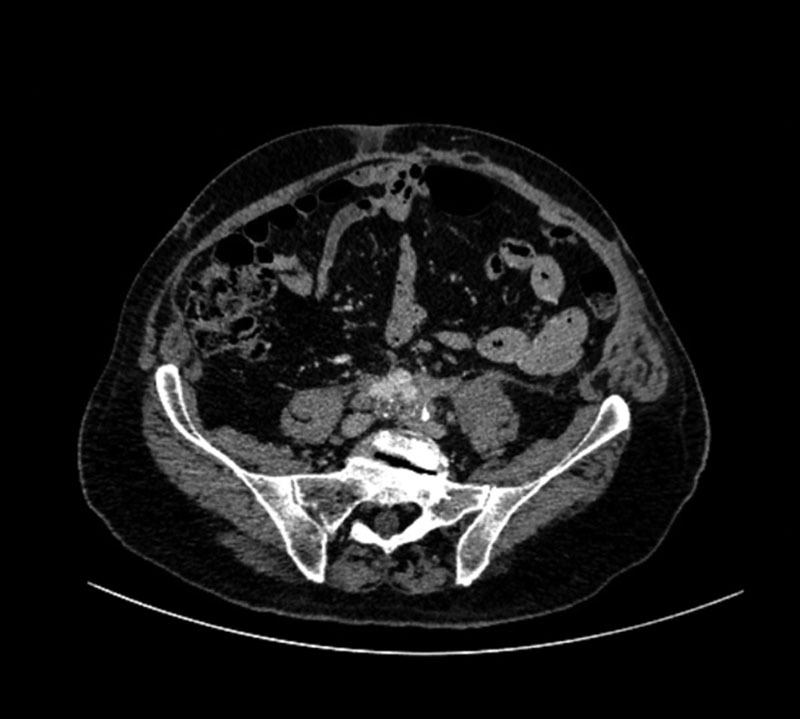
Tissue expanders are known adjuncts in ventral hernia repair, used in a staged approach where tissue closure or coverage of the defect is preferred but inadequate. Placement of tissue expanders in the correct tissue plane can be difficult, especially in thin patients or with loss of domain. This case series describes a technique in which tissue expander placement is facilitated by ultrasound-guided hydro-dissection, following the placement of a transversus abdominis plane (TAP) block. In short, after induction of anesthesia, the same needle used for the ultrasound-guided TAP block can be repositioned by the anesthesiologist to instill tumescent solution into the fascial plane between the internal and external oblique muscles. This allows for identification of the fascial planes in the ensuing operation. Our technique may prove to be an alternative tool in the placement of tissue expanders for ventral hernia repair, or in other procedures requiring device placement.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures

Similar articles
-
Laparoscopically assisted components separation technique for ventral incisional hernia repair.Hernia. 2007 Apr;11(2):157-61. doi: 10.1007/s10029-006-0175-2. Epub 2007 Jan 11. Hernia. 2007. PMID: 17216395
-
Ultrasound-guided transversus abdominis plane block: A technically easier analgesic option in obese compared to epidural.Anesth Essays Res. 2012 Jul-Dec;6(2):226-8. doi: 10.4103/0259-1162.108344. Anesth Essays Res. 2012. PMID: 25885625 Free PMC article.
-
Utility of ultrasound-guided transversus abdominis plane block for day-case inguinal hernia repair.Korean J Anesthesiol. 2017 Feb;70(1):46-51. doi: 10.4097/kjae.2017.70.1.46. Epub 2016 Oct 25. Korean J Anesthesiol. 2017. PMID: 28184266 Free PMC article.
-
Systematic review of transversus abdominis release in complex abdominal wall reconstruction.Hernia. 2019 Feb;23(1):5-15. doi: 10.1007/s10029-018-1870-5. Epub 2018 Dec 11. Hernia. 2019. PMID: 30539311
-
Evolution of the transversus abdominis plane block and its role in postoperative analgesia.Best Pract Res Clin Anaesthesiol. 2014 Jun;28(2):117-26. doi: 10.1016/j.bpa.2014.04.001. Epub 2014 May 9. Best Pract Res Clin Anaesthesiol. 2014. PMID: 24993433 Review.
Cited by
-
Exploring Variable Approaches in Complex Hernia Repair: A Comprehensive Literature Review.Cureus. 2024 May 13;16(5):e60181. doi: 10.7759/cureus.60181. eCollection 2024 May. Cureus. 2024. PMID: 38868245 Free PMC article. Review.
References
-
- de Vries Reilingh TS, Bodegom ME, van Goor H, et al. Autologous tissue repair of large abdominal wall defects. Br J Surg. 2007;94:791–803. - PubMed
-
- Luijendijk RW, Hop WC, van den Tol MP, et al. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med. 2000;343:392–398. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous