

A Classification for the Anterior Inferior Cerebellar Artery-Subarcuate Artery Complex Based on the Embryological Development
- PMID: 33134020
- PMCID: PMC7591361
- DOI: 10.1055/s-0039-1692474
A Classification for the Anterior Inferior Cerebellar Artery-Subarcuate Artery Complex Based on the Embryological Development
Abstract
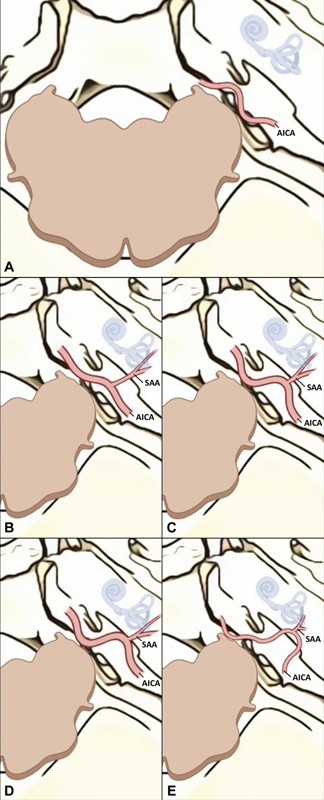
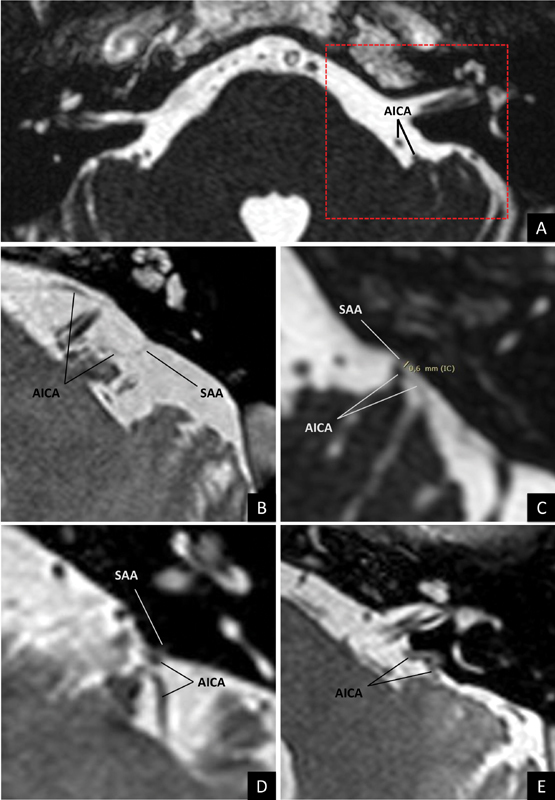
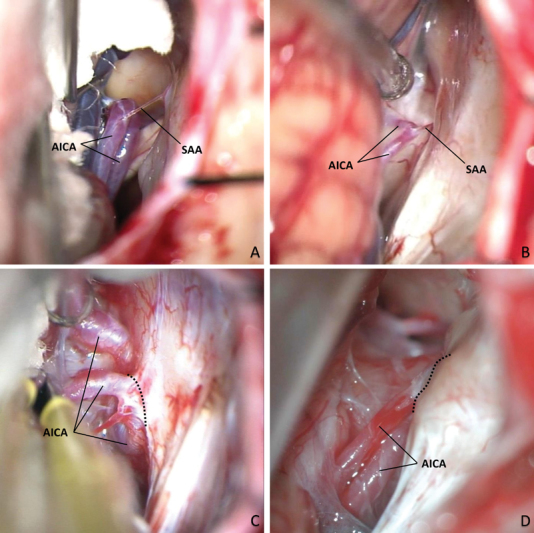
Objective To hierarchize the anterior inferior cerebellar artery (AICA)-subarcuate artery (SAA) complex's variations in the surgical field. Background The AICA's "subarcuate loop" (SL) presents multiple variations, closely related to the SAA. AICA-SAA complex's variations may represent major issues in cerebellopontine angle (CPA) surgery. As the spectrum of configurations is originated during the development, a systematized classification was proposed based on the interaction between the petrosal bone and the AICA in the embryonic period. Methods The variations were defined as follow: Grade 0: free, purely cisternal AICA, unidentifiable or absent SAA; Grade 1: purely cisternal AICA, loose SL, SAA > 3 mm; Grade 2: AICA near the subarcuate fossa, pronounced SL, SAA <3 mm; Grade 3: "duralized" AICA, unidentifiable SAA, or included in the petromastoid canal (PMC); and Grade 4: intraosseous AICA, unidentifiable SAA, or included in the PMC. The classification was applied to a series of patients assessed by magnetic resonance constructive interference in steady state sequence. Surgical examples were also provided. Results Eighty-four patients were evaluated, including 161 CPA. The proportions found in the gradation remained within the range of previous publications (Grade 0: 42.2%; Grade 1: 11.2%; Grade 2: 35.4%; Grade 3: 10.6%; and Grade 4: 0.6%). Moreover, the degrees of the classification were related to the complexity of the anatomical relationships and, therefore, to the difficulty of the maneuvers required to overcome them. Conclusion The proposed AICA-SAA complex classification allowed to distinguish and objectify pre- and intraoperatively the spectrum of variations, to thoroughly plan the required actions and instrumentation.
Keywords: anterior inferior cerebellar artery; cerebellopontine angle; petromastoid canal; subarcuate artery; subarcuate fossa; subarcuate loop.
© Thieme Medical Publishers.
Conflict of interest statement
Conflict of Interest None.
Figures
Similar articles
-
The Intraosseous Subarcuate Loop of Anterior Inferior Cerebellar Artery: Anatomic Management Guide, Single-Center MRI Study, and Scoping Review.Oper Neurosurg. 2024 Dec 23;29(3):389-398. doi: 10.1227/ons.0000000000001474. Oper Neurosurg. 2024. PMID: 39716468
-
Challenging Anterior Inferior Cerebellar Artery in Retrosigmoid Vestibular Schwannoma Removal.World Neurosurg. 2019 Jan;121:e370-e378. doi: 10.1016/j.wneu.2018.09.111. Epub 2018 Sep 25. World Neurosurg. 2019. PMID: 30261396
-
The anteroinferior cerebellar artery embedded in the subarcuate fossa: a rare anomaly and its clinical significance.Neurosurgery. 2005 Aug;57(2):314-9; discussion 314-9. doi: 10.1227/01.neu.0000166677.70797.5e. Neurosurgery. 2005. PMID: 16094161
-
The Anterior Inferior Cerebral Artery Variability in the Context of Neurovascular Compression Syndromes: A Narrative Review.Biomedicines. 2024 Feb 17;12(2):452. doi: 10.3390/biomedicines12020452. Biomedicines. 2024. PMID: 38398054 Free PMC article. Review.
-
Radiosurgery-Induced Anterior Inferior Cerebellar Artery Pseudoaneurysm Treated with Trapping and Bypass.World Neurosurg. 2018 Aug;116:209-213. doi: 10.1016/j.wneu.2018.04.161. Epub 2018 May 3. World Neurosurg. 2018. PMID: 29729463 Review.
Cited by
-
Management of a challenging dura-embedded anterior inferior cerebellar artery loop during a retrosigmoid hearing-preserving vestibular schwannoma resection: microsurgical technique and operative video. Illustrative case.J Neurosurg Case Lessons. 2023 Aug 21;6(8):CASE23304. doi: 10.3171/CASE23304. Print 2023 Aug 21. J Neurosurg Case Lessons. 2023. PMID: 37728311 Free PMC article.
-
The "Deep Subarcuate Fossa" sign and three types of anomalous subarcuate loops encountered during vestibular schwannoma removal.Acta Neurochir (Wien). 2022 Sep;164(9):2483-2490. doi: 10.1007/s00701-022-05288-6. Epub 2022 Jul 1. Acta Neurochir (Wien). 2022. PMID: 35776221
-
Emergent Revascularization After Transposition of an Unexpected Intraosseous Anomalous Subarcuate Loop During Vestibular Schwannoma Surgery: A Case Report.Neurosurg Pract. 2023 Jun 12;4(3):e00045. doi: 10.1227/neuprac.0000000000000045. eCollection 2023 Sep. Neurosurg Pract. 2023. PMID: 39958796 Free PMC article.
References
-
- Rhoton A L., JrThe cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach Neurosurgery 200047(3, Suppl):S93–S129. - PubMed
-
- Rhoton A L, Jr, Tedeschi H.Microsurgical anatomy of acoustic neuroma. 2002 Neurosurg Clin N Am 20081902145–174., v - PubMed
-
- Tatagiba M. Stuttgart, Germany: Springer; 2014. Retrosigmoid approach to the posterior and middle fossa; pp. 217–235.
-
- Martin R G, Grant J L, Peace D, Theiss C, Rhoton A L., Jr Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery. 1980;6(05):483–507. - PubMed
-
- Rhoton A L., JrThe cerebellar arteries Neurosurgery 200047(3, Suppl):S29–S68. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
