

Endoscopic Endonasal Transpterygoid Approach to Sphenoid Sinus Lateral Recess Defects
- PMID: 33134022
- PMCID: PMC7591366
- DOI: 10.1055/s-0039-1692639
Endoscopic Endonasal Transpterygoid Approach to Sphenoid Sinus Lateral Recess Defects
Abstract
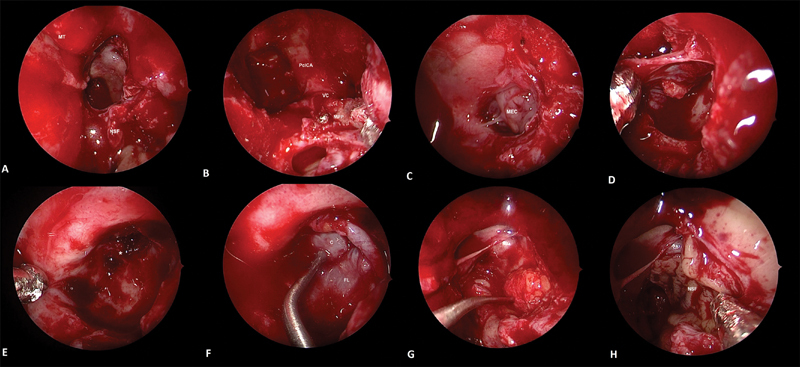
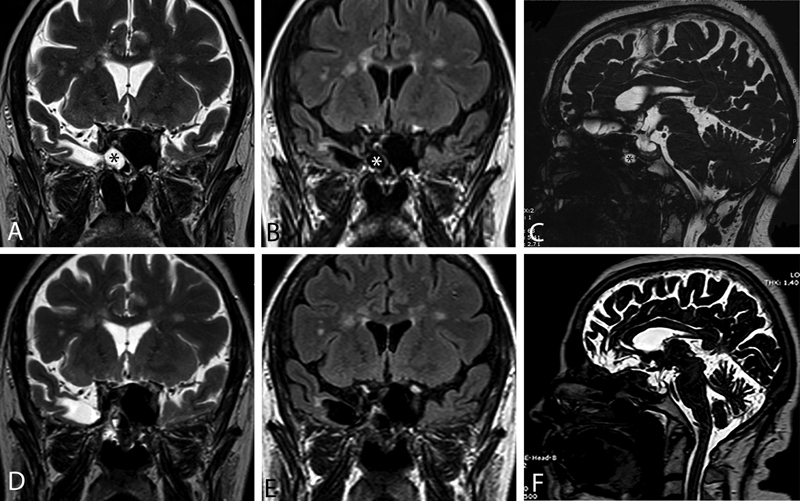
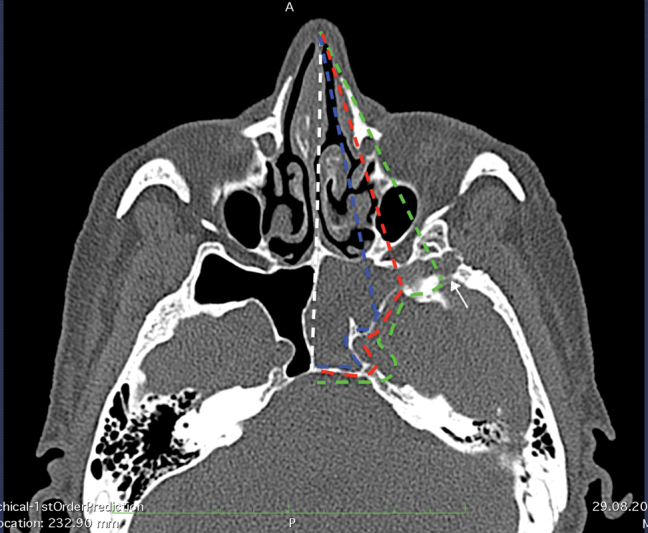
Background Lesions affecting sphenoid sinus lateral recess (SSLR) are difficult to visualize and manipulate through the transnasal routes, especially when the sinus is highly pneumatized. External approaches to this area involve extensive surgery and are associated with significant morbidity. The aims of this study are to present our experience with the endoscopic transpterygoid approach as a method for approaching lesions of the SSLR and to evaluate the outcomes of this procedure. Methods Clinical charts of patients who had lesions in the SSLR and who were treated at our institution from September 1998 to June 2018 were retrospectively reviewed. All these patients were managed by the endoscopic endonasal transpterygoid approach. Results Thirty-nine patients were identified. No cerebrospinal fluid leak recurrences were observed during follow-up (range: 1-19.7 years; median: 2.3 years). Hypoesthesia (temporary, 1; persistent, 4) in the region innervated by the maxillary branch of the trigeminal nerve was detected in five (12.8%) patients, while symptoms due to the Vidian nerve damage (dry eye, 3; dry nasal mucosa, 1) were present in four (10%) patients. Conclusions Although the endoscopic endonasal transpterygoid approach is an excellent corridor for dealing with lesions of the SSLR, limited rate of neurologic and lacrimal complications was observed. Potential morbidity of the intervention should be discussed during preoperative counselling.
Keywords: cerebrospinal fluid leak; endoscopic transpterygoid approach; meningoencephalocele; skull base; sphenoid sinus lateral recess.
© Thieme Medical Publishers.
Conflict of interest statement
Conflicts of Interest There are no conflicts of interest.
Figures

Similar articles
-
Surgical Management of Sphenoid Sinus Lateral Recess Cerebrospinal Fluid Leaks: A Single Neurosurgical Center Analysis of Endoscopic Endonasal Minimal Transpterygoid Approach.World Neurosurg. 2018 Oct;118:e473-e482. doi: 10.1016/j.wneu.2018.06.219. Epub 2018 Jul 6. World Neurosurg. 2018. PMID: 29981913
-
[Experience of treating patients with lateral sphenoid sinus recess CSF leak].Zh Vopr Neirokhir Im N N Burdenko. 2018;82(6):68-75. doi: 10.17116/neiro20188206168. Zh Vopr Neirokhir Im N N Burdenko. 2018. PMID: 30721219 Russian.
-
Management of Cerebrospinal Fluid Rhinorrhea in the Sphenoid Sinus Lateral Recess Through an Endoscopic Endonasal Transpterygoid Approach With Obliteration of the Lateral Recess.Ear Nose Throat J. 2022 Jun;101(5):319-325. doi: 10.1177/0145561320955140. Epub 2020 Sep 13. Ear Nose Throat J. 2022. PMID: 32921179
-
[Endoscopic transpterygoid intervention for lesions of lateral recess of sphenoid sinus in 4 cases(with literature review) ].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019 May;33(5):411-415. doi: 10.13201/j.issn.1001-1781.2019.05.007. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2019. PMID: 31163547 Review. Chinese.
-
Surgical nuances for the endoscopic endonasal transpterygoid approach to lateral sphenoid sinus encephaloceles.Neurosurg Focus. 2012 Jun;32(6):E5. doi: 10.3171/2012.3.FOCUS1267. Neurosurg Focus. 2012. PMID: 22655694 Review.
Cited by
-
Endoscopic endonasal access to the lateral recess of the sphenoid sinus.Acta Neurochir (Wien). 2023 Dec;165(12):4113-4119. doi: 10.1007/s00701-023-05856-4. Epub 2023 Oct 27. Acta Neurochir (Wien). 2023. PMID: 37889336
-
Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Endoscopic Endonasal and Endoscopic-Assisted Transmaxillary Transpterygoid Approaches.J Neurol Surg B Skull Base. 2022 Dec 28;85(1):81-94. doi: 10.1055/s-0042-1759874. eCollection 2024 Feb. J Neurol Surg B Skull Base. 2022. PMID: 38274480 Free PMC article.
-
Endoscopic endonasal repair of temporal lobe meningoencephalocele in the lateral recess of the sphenoid sinus, complicated by intracerebral hematoma: illustrative case.J Neurosurg Case Lessons. 2023 Dec 25;6(26):CASE23575. doi: 10.3171/CASE23575. Print 2023 Dec 25. J Neurosurg Case Lessons. 2023. PMID: 38145563 Free PMC article.
-
Endonasal endoscopic surgery for temporal lobe epilepsy associated with sphenoidal encephalocele.Surg Neurol Int. 2021 Jul 27;12:379. doi: 10.25259/SNI_542_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34513146 Free PMC article.
-
Quantitative Anatomical Comparison of Surgical Approaches to Meckel's Cave.J Clin Med. 2023 Oct 30;12(21):6847. doi: 10.3390/jcm12216847. J Clin Med. 2023. PMID: 37959312 Free PMC article.
References
-
- Vaezi A, Cardenas E, Pinheiro-Neto C. Classification of sphenoid sinus pneumatization: relevance for endoscopic skull base surgery. Laryngoscope. 2015;125(03):577–581. - PubMed
-
- Martínez-Capoccioni G, Serramito-García R, Huertas-Pardo B, García-Allut A, Martín-Martín C. Spontaneous cerebrospinal fluid leaks in the anterior skull base: a surgical challenge. J Laryngol Otol. 2015;129(04):358–364. - PubMed
-
- Lai S Y, Kennedy D W, Bolger W E. Sphenoid encephaloceles: disease management and identification of lesions within the lateral recess of the sphenoid sinus. Laryngoscope. 2002;112(10):1800–1805. - PubMed
-
- Woodworth B A, Prince A, Chiu A G. Spontaneous CSF leaks: a paradigm for definitive repair and management of intracranial hypertension. Otolaryngol Head Neck Surg. 2008;138(06):715–720. - PubMed
-
- Aggarwal V, Nair P, Shivhare P. A case of evolving bilateral sphenoidal meningoencephaloceles: case report and review of the literature. World Neurosurg. 2017;100:7.08E13–7.08E19. - PubMed
