

The 2-Scope Technique for Rotator Cuff Surgery: Are 2 Scopes Better Than 1?
- PMID: 33134065
- PMCID: PMC7587691
- DOI: 10.1016/j.eats.2020.06.025
The 2-Scope Technique for Rotator Cuff Surgery: Are 2 Scopes Better Than 1?
Abstract
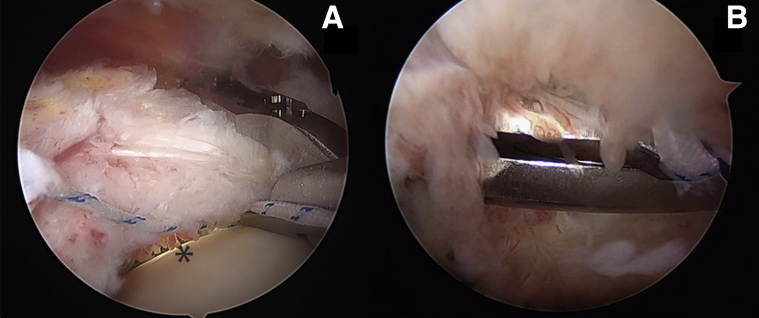
The arthroscopic treatment of rotator cuff tear involves 2 distinct phases: intra-articular and subacromial. We present the 2-scope technique with the aim to simultaneously perform these phases, entrusting them to 2 experienced surgeons, and to obtain possible benefits compared with the classic 1-scope technique. Better nosology of the lesion and a more accurate evaluation of suture passer action (equidistance of the sutures and avoidance of degenerated articular-side tendon areas) represent benefits of this technique. In contrast, the 2-scope technique needs an additional lateral portal and could give rise to an erroneous distribution of costs and surgeons.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures






References
-
- Snyder S.J. Shoulder arthroscopy. 2nd ed. JB Lippincott; Philadelphia: 2002. Arthroscopic classification of rotator cuff lesions and surgical decision making; p. 204.
-
- Davidson J., Burkhart S.S. The geometric classification of rotator cuff tears: A system linking tear pattern to treatment and prognosis. Arthroscopy. 2010;26:417–424. - PubMed
-
- Gumina S., Borroni M. Rotator cuff tear. Pathogenesis, evaluation and treatment. Springer International; Cham: 2017. Classifications of rotator cuff tears; pp. 123–131.
-
- Habermeyer P., Krieter C., Tang K.I., Lichtenberg S., Magosh P. A new arthroscopic classification of articular-sided supraspinatus footprint lesions: A prospective comparison with Snyder’s and Ellman’s classification. J Shoulder Elbow Surg. 2008;17:909–913. - PubMed
LinkOut - more resources
Full Text Sources
