

Arthroscopic Transosseous Suture-bridge Fixation for Anterior Cruciate Ligament Tibial Avulsion Fractures
- PMID: 33134068
- PMCID: PMC7586735
- DOI: 10.1016/j.eats.2020.05.005
Arthroscopic Transosseous Suture-bridge Fixation for Anterior Cruciate Ligament Tibial Avulsion Fractures
Abstract
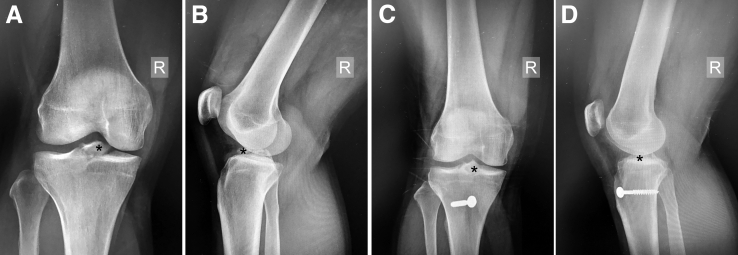
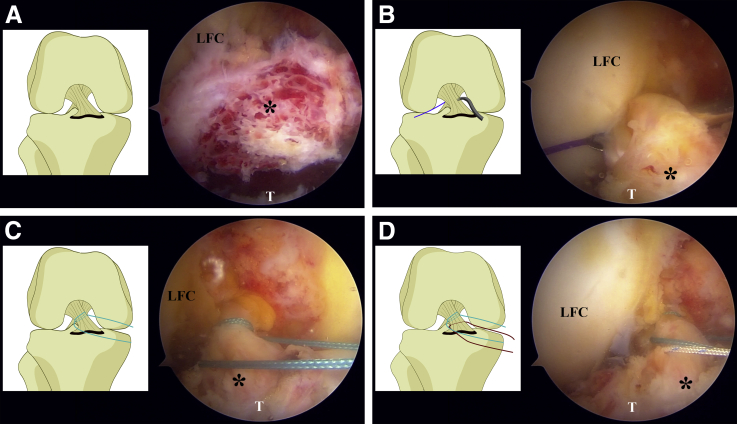
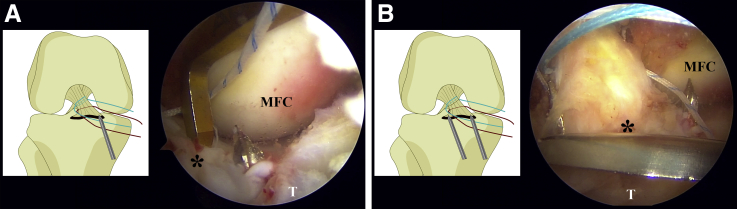
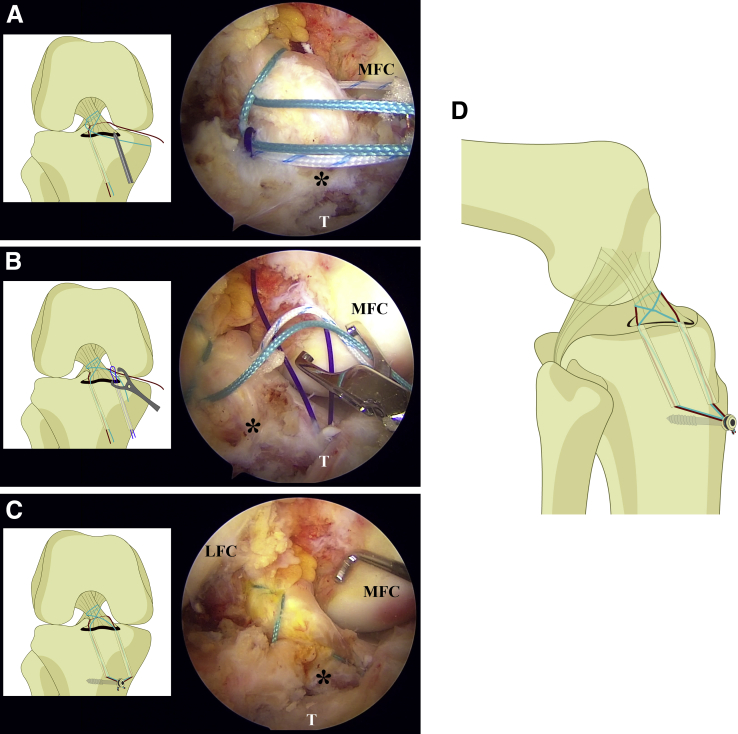
Few cases of tibial spine avulsion injuries occur in adolescents. An open or arthroscopic surgical approach is indicated for displaced and nonreducible fractures, but evidence for a gold standard is insufficient. Various arthroscopic techniques are available. Suture fixation is popular and shows good results. The proposed technique is a modified suture-bridge fixation using 2 high-strength sutures tied through 2 transosseous tunnels. This simple and low-cost technique avoids the potential complications of hardware fixation within a joint. It represents an arthroscopic treatment option for anterior cruciate ligament tibial avulsion injuries.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
References
-
- Skak S.V., Jensen T.T., Poulsen T.D., Sturup J. Epidemiology of knee injuries in children. Acta Orthop Scand. 1987;58:78–81. - PubMed
-
- Meyers M.H., McKeever F.M. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1970;52:1677–1684. - PubMed
-
- Zaricznyj B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59:1111–1114. - PubMed
-
- Gans I., Baldwin K.D., Ganley T.J. Treatment and management outcomes of tibial eminence fractures in pediatric patients: A systematic review. Am J Sports Med. 2014;42:1743–1750. - PubMed
-
- Furlan D., Pogorelic Z., Biocic M., Juric I., Mestrovic J. Pediatric tibial eminence fractures: Arthroscopic treatment using K-wire. Scand J Surg. 2010;99:38–44. - PubMed
LinkOut - more resources
Full Text Sources
