

Restoring Horizontal Stability of the Acromioclavicular Joint: Open Acromioclavicular Ligament Reconstruction and Repair With Semitendinosus Allograft
- PMID: 33134070
- PMCID: PMC7587926
- DOI: 10.1016/j.eats.2020.07.002
Restoring Horizontal Stability of the Acromioclavicular Joint: Open Acromioclavicular Ligament Reconstruction and Repair With Semitendinosus Allograft
Abstract
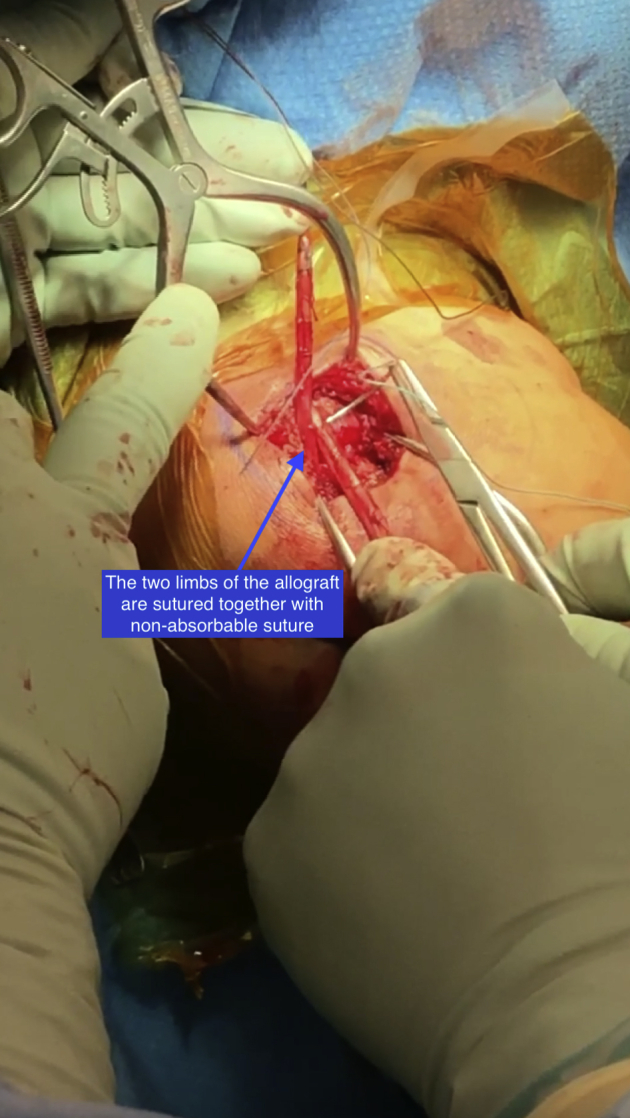
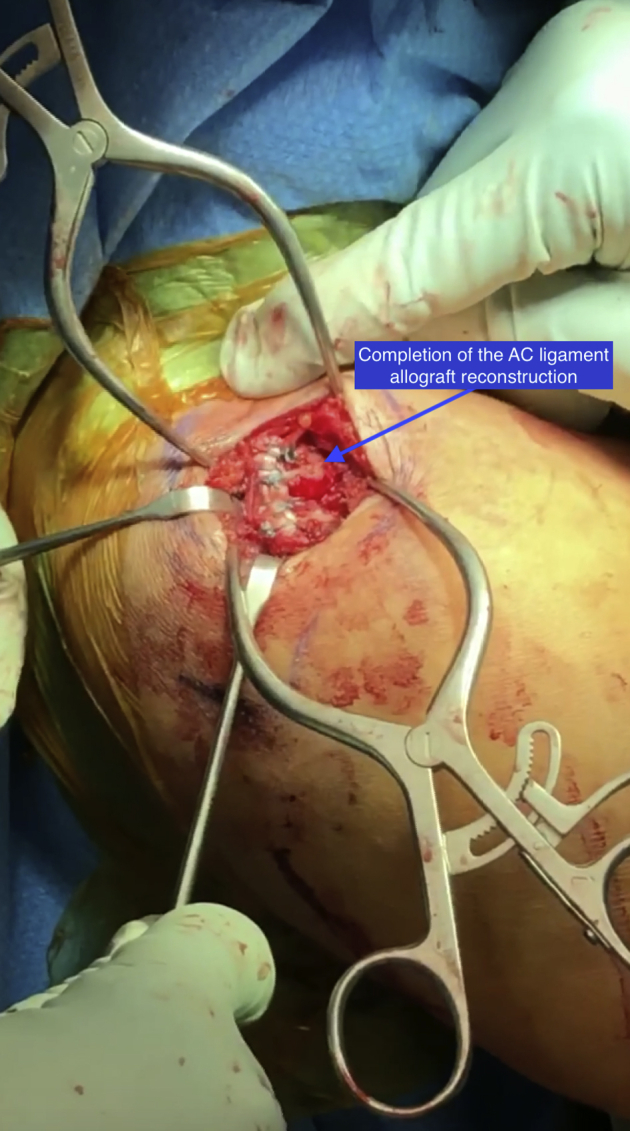
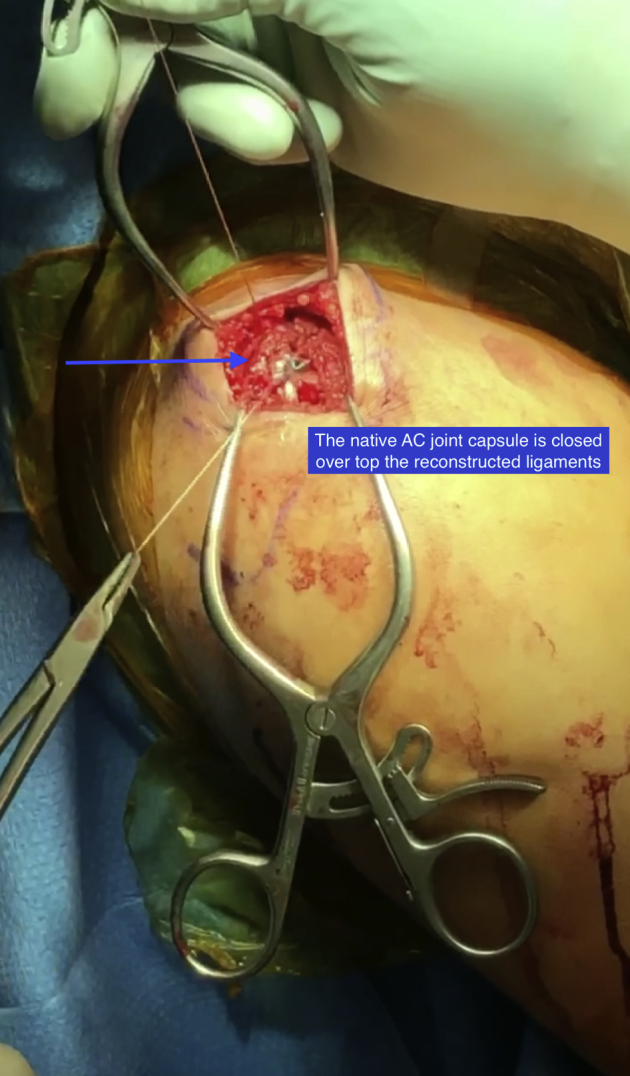
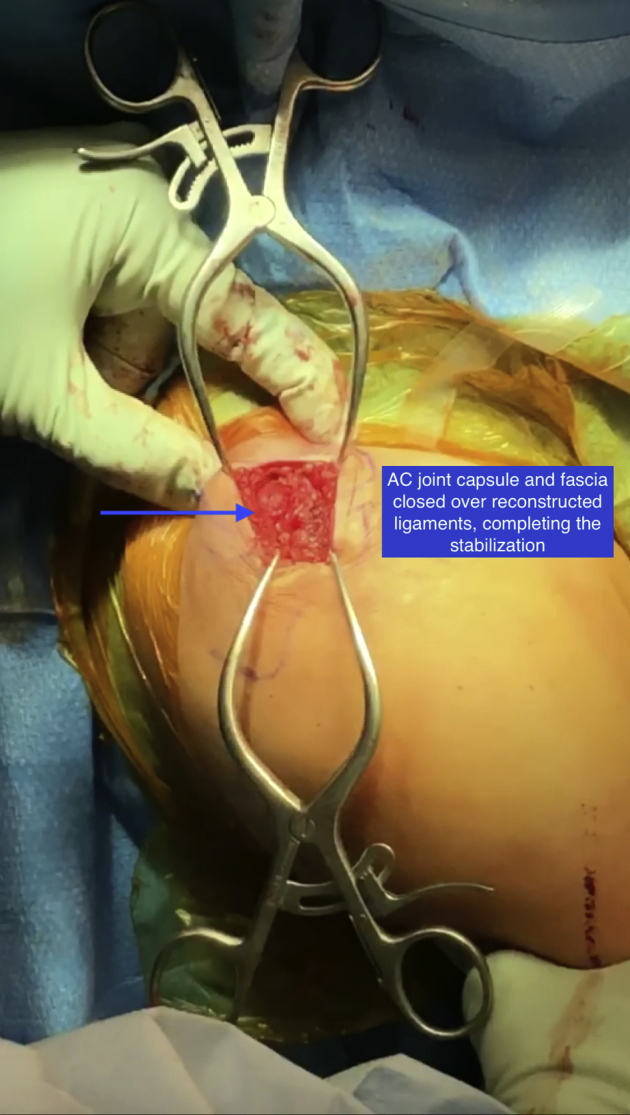
Injuries to the acromioclavicular (AC) joint are common and comprise ∼12% of shoulder injuries. Stability to the AC joint depends on the coracoclavicular (CC) ligaments for vertical stability and AC ligaments and capsular structures for horizontal stability. Injuries to the AC ligaments can lead to horizontal instability of the AC joint. There is no gold standard technique for treating these injuries surgically, and many of the described procedures focus on vertical instability rather than horizontal instability. This article describes an open AC ligament reconstruction with semitendinosus allograft to restore horizontal stability of the AC joint.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
References
-
- Braun S., Imhoff A.B., Martetschlaeger F. Primary fixation of acromioclavicular joint disruption. Oper Tech Sports Med. 2014;22:221–226.
-
- Li X., Ma R., Bedi A., Dines D.M., Altchek D.W., Dines J.S. Management of acromioclavicular joint injuries. J Bone Joint Surg Am. 2014;96:73–84. - PubMed
-
- Dyrna F.G.E., Imhoff F.B., Voss A. The integrity of the acromioclavicular capsule ensures physiological centering of the acromioclavicular joint under rotational loading. Am J Sports Med. 2018;46:1432–1440. - PubMed
LinkOut - more resources
Full Text Sources
