

Dosimetric Impact of the Positional Imaging Frequency for Hypofractionated Prostate Radiotherapy - A Voxel-by-Voxel Analysis
- PMID: 33134166
- PMCID: PMC7550661
- DOI: 10.3389/fonc.2020.564068
Dosimetric Impact of the Positional Imaging Frequency for Hypofractionated Prostate Radiotherapy - A Voxel-by-Voxel Analysis
Abstract
Background: To investigate deviations between planned and applied treatment doses for hypofractionated prostate radiotherapy and to quantify dosimetric accuracy in dependence of the image guidance frequency.
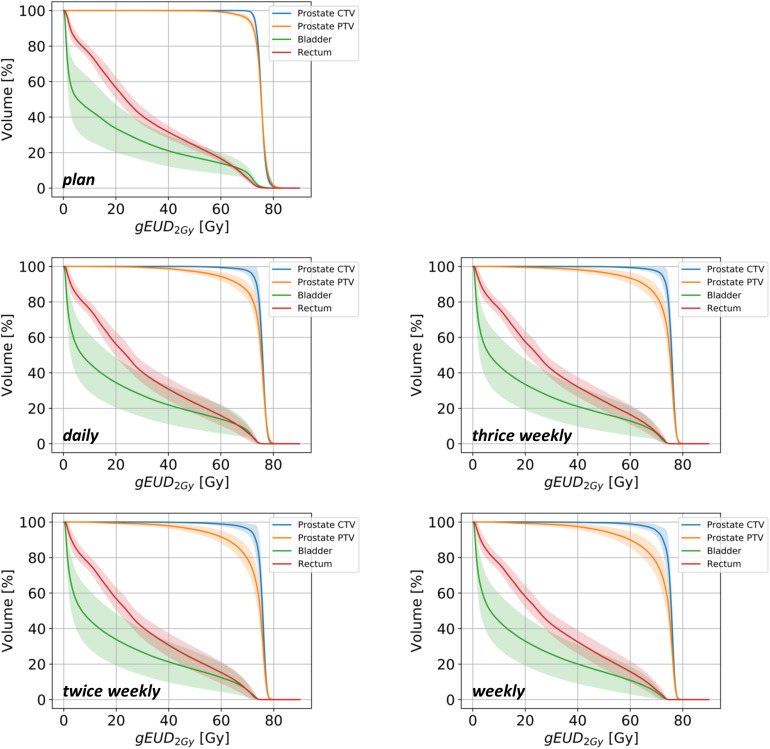
Methods: Daily diagnostic in-room CTs were carried out in 10 patients in treatment position as image guidance for hypofractionated prostate radiotherapy. Fraction doses were mapped to the planning CTs and recalculated, and applied doses were accumulated voxel-wise using deformable registration. Non-daily imaging schedules were simulated by deriving position correction vectors from individual scans and used to rigidly register the following scans until the next repositioning before dose recalculation and accumulation. Planned and applied doses were compared regarding dose-volume indices and TCP and NTCP values in dependence of the imaging and repositioning frequency.
Results: Daily image-guided repositioning was associated with only negligible deviations of analyzed dose-volume parameters and conformity/homogeneity indices for the prostate, bladder and rectum. Average CTV T did not significantly deviate from the plan values, and rectum NTCPs were highly comparable, while bladder NTCPs were reduced. For non-daily image-guided repositioning, there were significant deviations in the high-dose range from the planned values. Similarly, CTV dose conformity and homogeneity were reduced. While TCPs and rectal NTCPs did not significantly deteriorate for non-daily repositioning, bladder NTCPs appeared falsely diminished in dependence of the imaging frequency.
Conclusion: Using voxel-by-voxel dose accumulation, we showed for the first time that daily image-guided repositioning resulted in only negligible dosimetric deviations for hypofractionated prostate radiotherapy. Regarding dosimetric aberrations for non-daily imaging, daily imaging is required to adequately deliver treatment.
Keywords: dosimetry; hypofractionation; image-guided radiotherapy; organs-at-risk; prostate cancer; tumor control probability.
Copyright © 2020 Splinter, Sachpazidis, Bostel, Fechter, Zamboglou, Thieke, Jäkel, Huber, Debus, Baltas and Nicolay.
Figures




References
-
- Kupelian PA, Potters L, Khuntia D, Ciezki JP, Reddy CA, Reuther AM, et al. Radical prostatectomy, external beam radiotherapy or =72 Gy, permanent seed implantation, or combined seeds/external beam radiotherapy for stage T1-T2 prostate cancer. Int J Radiat Oncol Biol Phys. (2004) 58:25–33. 10.1016/S0360-3016(03)00784-3 - DOI - PubMed
-
- Viani GA, Viana BS, Martin JE, Rossi BT, Zuliani G, Stefano EJ. Intensity-modulated radiotherapy reduces toxicity with similar biochemical control compared with 3-dimensional conformal radiotherapy for prostate cancer: a randomized clinical trial. Cancer. (2016) 122:2004–11. 10.1002/cncr.29983 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials