

Management of Gram-Negative Bloodstream Infections in the Era of Rapid Diagnostic Testing: Impact With and Without Antibiotic Stewardship
- PMID: 33134414
- PMCID: PMC7585329
- DOI: 10.1093/ofid/ofaa427
Management of Gram-Negative Bloodstream Infections in the Era of Rapid Diagnostic Testing: Impact With and Without Antibiotic Stewardship
Abstract
Background: Verigene Blood-Culture Gram-Negative is a rapid diagnostic test (RDT) that detects gram-negatives (GNs) and resistance within hours from gram stain. The majority of the data support the use of RDTs with antimicrobial stewardship (AMS) intervention in gram-positive bloodstream infection (BSI). Less is known about GN BSI.
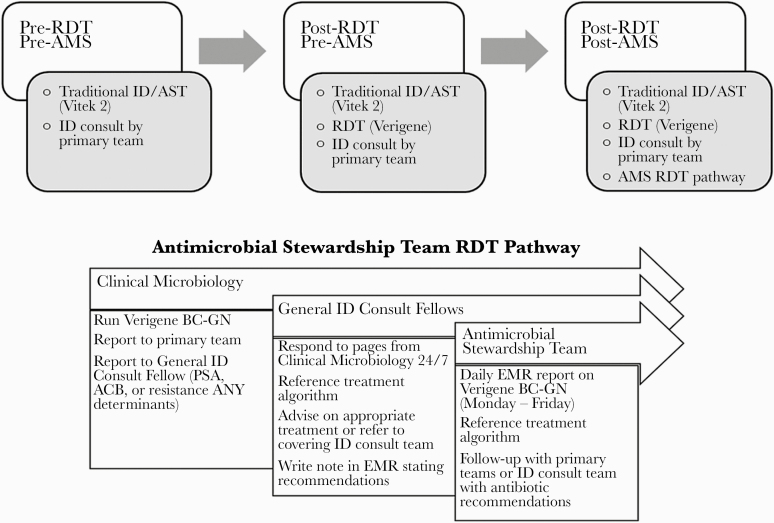
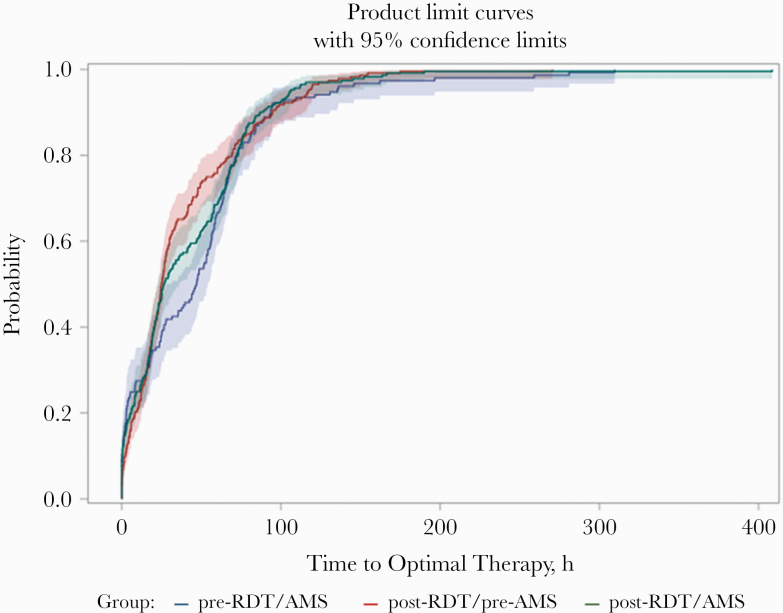
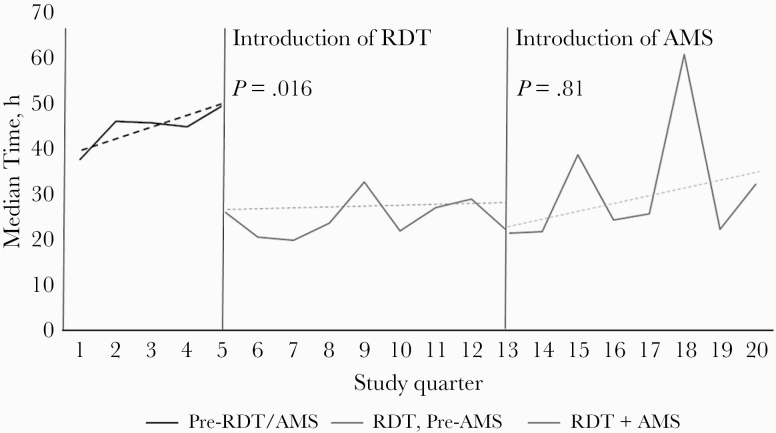
Methods: This was a retrospective quasi-experimental (nonrandomized) study of adult patients with RDT-target GN BSI comparing patients pre-RDT/AMS vs post-RDT/pre-AMS vs post-RDT/AMS. Optimal therapy was defined as appropriate coverage with the narrowest spectrum, accounting for source and co-infecting organisms. Time to optimal therapy was analyzed using Kaplan-Meier and multivariable Cox proportional hazards regression.
Results: Eight-hundred thirty-two patients were included; 237 pre-RDT/AMS vs 308 post-RDT/pre-AMS vs 237 post-RDT/AMS, respectively. The proportion of patients on optimal antibiotic therapy increased with each intervention (66.5% vs 78.9% vs 83.2%; P < .0001). Time to optimal therapy (interquartile range) decreased with introduction of RDT: 47 (7.9-67.7) hours vs 24.9 (12.4-55.2) hours vs 26.5 (10.3-66.5) hours (P = .09). Using multivariable modeling, infectious diseases (ID) consult was an effect modifier. Within the ID consult stratum, controlling for source and ICU stay, compared with the pre-RDT/AMS group, both post-RDT/pre-AMS (adjusted hazard ratio [aHR], 1.34; 95% CI, 1.04-1.72) and post-RDT/AMS (aHR, 1.28; 95% CI, 1.01-1.64), improved time to optimal therapy. This effect was not seen in the stratum without ID consult.
Conclusions: With the introduction of RDT and AMS, both proportion and time to optimal antibiotic therapy improved, especially among those with an existing ID consult. This study highlights the beneficial role of RDTs in GN BSI.
Keywords: antimicrobial stewardhip; gram-negative bloodstream infection; rapid diagnostic testing.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
Similar articles
-
Implementation of a Rapid Phenotypic Susceptibility Platform for Gram-Negative Bloodstream Infections With Paired Antimicrobial Stewardship Intervention: Is the Juice Worth the Squeeze?Clin Infect Dis. 2021 Sep 7;73(5):783-792. doi: 10.1093/cid/ciab126. Clin Infect Dis. 2021. PMID: 33580233 Free PMC article.
-
Rapid testing using the Verigene Gram-negative blood culture nucleic acid test in combination with antimicrobial stewardship intervention against Gram-negative bacteremia.Antimicrob Agents Chemother. 2015 Mar;59(3):1588-95. doi: 10.1128/AAC.04259-14. Epub 2014 Dec 29. Antimicrob Agents Chemother. 2015. PMID: 25547353 Free PMC article.
-
Impact of a Rapid Blood Culture Diagnostic Test in a Children's Hospital Depends on Gram-Positive versus Gram-Negative Organism and Day versus Night Shift.J Clin Microbiol. 2020 Mar 25;58(4):e01400-19. doi: 10.1128/JCM.01400-19. Print 2020 Mar 25. J Clin Microbiol. 2020. PMID: 31852761 Free PMC article.
-
The Use of Bloodstream Infection Mortality to Measure the Impact of Antimicrobial Stewardship Interventions: Assessing the Evidence.Infect Dis Rep. 2017 Mar 30;9(1):6849. doi: 10.4081/idr.2017.6849. eCollection 2017 Mar 30. Infect Dis Rep. 2017. PMID: 28458799 Free PMC article. Review.
-
Antimicrobial Stewardship in Tropical Infectious Diseases: Focusing on Dengue and Malaria.Trop Med Infect Dis. 2022 Jul 30;7(8):159. doi: 10.3390/tropicalmed7080159. Trop Med Infect Dis. 2022. PMID: 36006251 Free PMC article. Review.
Cited by
-
A comparison of active versus passive methods of responding to rapid diagnostic blood culture results.Antimicrob Steward Healthc Epidemiol. 2022 May 2;2(1):e75. doi: 10.1017/ash.2022.26. eCollection 2022. Antimicrob Steward Healthc Epidemiol. 2022. PMID: 36483427 Free PMC article.
-
Comparing the Clinical Utility of Rapid Diagnostics for Treatment of Bloodstream Infections Using Desirability of Outcome Ranking Approach for the Management of Antibiotic Therapy (DOOR-MAT).Antimicrob Agents Chemother. 2021 Aug 17;65(9):e0044121. doi: 10.1128/AAC.00441-21. Epub 2021 Aug 17. Antimicrob Agents Chemother. 2021. PMID: 34228533 Free PMC article.
-
Rapid diagnostic testing combined with an immediate infectious disease consultation increases the rate of septic intensive care unit patients on targeted antibiotic therapy.Front Cell Infect Microbiol. 2025 Jan 21;14:1513408. doi: 10.3389/fcimb.2024.1513408. eCollection 2024. Front Cell Infect Microbiol. 2025. PMID: 39906215 Free PMC article.
-
Rapid Diagnostic Tests and Antimicrobial Stewardship Programs for the Management of Bloodstream Infection: What Is Their Relative Contribution to Improving Clinical Outcomes? A Systematic Review and Network Meta-analysis.Clin Infect Dis. 2024 Aug 16;79(2):502-515. doi: 10.1093/cid/ciae234. Clin Infect Dis. 2024. PMID: 38676943 Free PMC article.
-
Impact of a Multistep Bundles Intervention in the Management and Outcome of Gram-Negative Bloodstream Infections: A Single-Center "Proof-of-Concept" Study.Open Forum Infect Dis. 2022 Sep 17;9(10):ofac488. doi: 10.1093/ofid/ofac488. eCollection 2022 Oct. Open Forum Infect Dis. 2022. PMID: 36267259 Free PMC article.
References
-
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect 2013; 19:501–9. - PubMed
-
- Centers for Disease Control and Prevention. The biggest antibiotic-resistant threats in the U.S. Centers for Disease Control and Prevention. 2018 Available at: https://www.cdc.gov/drugresistance/biggest_threats.html. Accessed 24 February 2019.
-
- Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest 2000; 118:146–55. - PubMed
