

Longitudinal Progression of Subclinical Coronary Atherosclerosis in Swiss HIV-Positive Compared With HIV-Negative Persons Undergoing Coronary Calcium Score Scan and CT Angiography
- PMID: 33134415
- PMCID: PMC7585327
- DOI: 10.1093/ofid/ofaa438
Longitudinal Progression of Subclinical Coronary Atherosclerosis in Swiss HIV-Positive Compared With HIV-Negative Persons Undergoing Coronary Calcium Score Scan and CT Angiography
Abstract
Background: People with HIV (HIV+) may have increased cardiovascular event rates compared with HIV-negative (HIV-) persons. Cross-sectional data from the United States and Switzerland, based on coronary artery calcium scan (CAC) and coronary computed tomography angiography (CCTA), suggest, respectively, increased and similar prevalence of subclinical atherosclerosis in HIV+ vs HIV- persons.
Methods: We repeated CAC/CCTA in 340 HIV+ and 90 HIV- study participants >2 years after baseline CAC/CCTA. We assessed the association of HIV infection, Framingham risk score (FRS), and HIV-related factors with the progression of subclinical atherosclerosis.
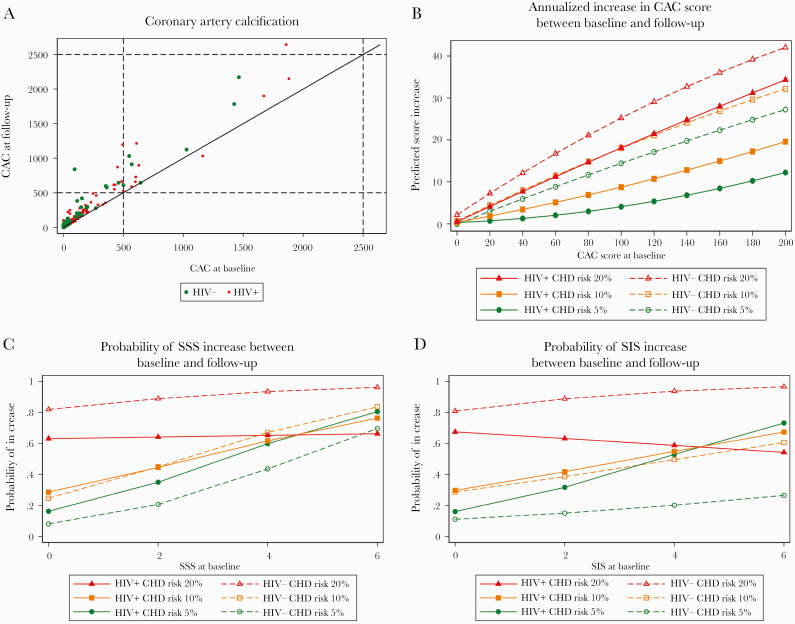
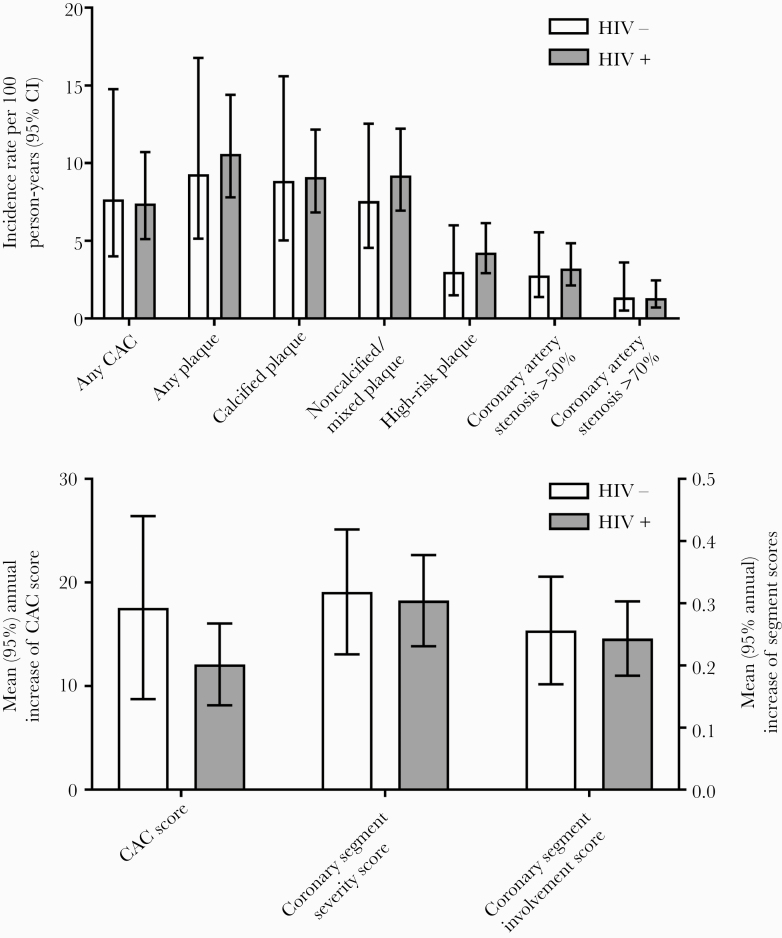
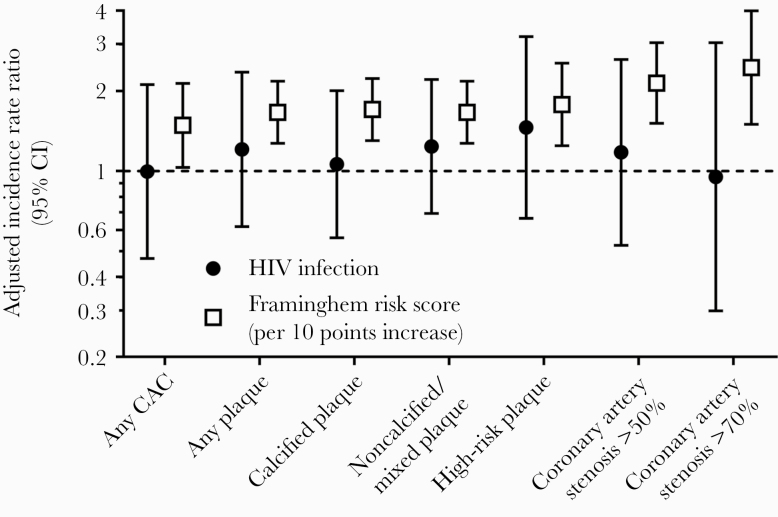
Results: HIV+ were younger than HIV- participants (median age, 52 vs 56 years; P < .01) but had similar median 10-year FRS (8.9% vs 9.0%; P = .82); 94% had suppressed HIV viral load. In univariable and multivariable analyses, FRS was associated with the incidence rate ratio (IRR) of new subclinical atherosclerosis at the follow-up CAC/CCTA, but HIV infection was not: any plaque (adjusted IRR for HIV+ vs HIV- participants, 1.21; 95% CI, 0.62-2.35), calcified plaque (adjusted IRR for HIV+ vs HIV- participants, 1.06; 95% CI, 0.56-2), noncalcified/mixed plaque (adjusted IRR for HIV+ vs HIV- participants, 1.24; 95% CI, 0.69-2.21), and high-risk plaque (adjusted IRR for HIV+ vs HIV- participants, 1.46; 95% CI, 0.66-3.20). Progression of CAC score between baseline and follow-up CAC/CCTA was similar in HIV+ (median annualized change [interquartile range {IQR}], 0.41 [0-10.19]) and HIV- participants (median annualized change [IQR], 2.38 [0-16.29]; P = .11), as was progression of coronary segment severity score (HIV+: median annualized change [IQR], 0 [0-0.47]; HIV-: median annualized change [IQR], 0 [0-0.52]; P = .10) and coronary segment involvement score (HIV+: median annualized change [IQR], 0 [0-0.45]; HIV-: median annualized change [IQR], 0 [0-0.41]; P = .25).
Conclusions: In this longitudinal CAC/CCTA study from Switzerland, Framingham risk score was associated with progression of subclinical atherosclerosis, but HIV infection was not.
Keywords: HIV; cardiovascular disease; coronary CT angiography; longitudinal study; subclinical atherosclerosis.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
Similar articles
-
Subclinical coronary artery disease in Swiss HIV-positive and HIV-negative persons.Eur Heart J. 2018 Jun 14;39(23):2147-2154. doi: 10.1093/eurheartj/ehy163. Eur Heart J. 2018. PMID: 29590332
-
Antiretroviral Drugs Associated With Subclinical Coronary Artery Disease in the Swiss Human Immunodeficiency Virus Cohort Study.Clin Infect Dis. 2020 Feb 14;70(5):884-889. doi: 10.1093/cid/ciz283. Clin Infect Dis. 2020. PMID: 30958888
-
Frailty and subclinical coronary atherosclerosis: The Multicenter AIDS Cohort Study (MACS).Atherosclerosis. 2017 Nov;266:240-247. doi: 10.1016/j.atherosclerosis.2017.08.026. Epub 2017 Aug 26. Atherosclerosis. 2017. PMID: 28886899 Free PMC article.
-
Bridging Prevention and Imaging: The Influence of Statins on CAC and CCTA Findings.Curr Atheroscler Rep. 2025 Apr 8;27(1):50. doi: 10.1007/s11883-025-01287-x. Curr Atheroscler Rep. 2025. PMID: 40198377 Review.
-
Subclinical Atherosclerosis Imaging in People Living with HIV.J Clin Med. 2019 Jul 29;8(8):1125. doi: 10.3390/jcm8081125. J Clin Med. 2019. PMID: 31362391 Free PMC article. Review.
Cited by
-
HIV indirectly accelerates coronary artery disease by promoting the effects of risk factors: longitudinal observational study.Sci Rep. 2021 Nov 30;11(1):23110. doi: 10.1038/s41598-021-02556-w. Sci Rep. 2021. PMID: 34848791 Free PMC article.
-
Sex modifies the association between HIV and coronary artery disease among older adults in Uganda.J Int AIDS Soc. 2022 Jan;25(1):e25868. doi: 10.1002/jia2.25868. J Int AIDS Soc. 2022. PMID: 34995413 Free PMC article.
-
Coronary Artery Calcification and Plaque Characteristics in People Living With HIV: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2021 Oct 5;10(19):e019291. doi: 10.1161/JAHA.120.019291. Epub 2021 Sep 29. J Am Heart Assoc. 2021. PMID: 34585590 Free PMC article.
-
Cardiovascular Risk in People Living with Human Immunodeficiency (HIV) Viremia Suppression in a Young, Mid-Eastern European Population - Preliminary Study.Vasc Health Risk Manag. 2024 Sep 21;20:435-445. doi: 10.2147/VHRM.S472328. eCollection 2024. Vasc Health Risk Manag. 2024. PMID: 39324108 Free PMC article.
-
Higher cardiovascular disease risks in people living with HIV: A systematic review and meta-analysis.J Glob Health. 2024 Apr 26;14:04078. doi: 10.7189/jogh.14.04078. J Glob Health. 2024. PMID: 38666515 Free PMC article.
References
-
- Worm SW, Sabin C, Weber R, et al. Risk of myocardial infarction in patients with HIV infection exposed to specific individual antiretroviral drugs from the 3 major drug classes: the data collection on adverse events of anti-HIV drugs (D:A:D) study. J Infect Dis 2010; 201:318–30. - PubMed
