

Hyponatremia Is Associated With Increased Mortality in Children on the Waiting List for Liver Transplantation
- PMID: 33134484
- PMCID: PMC7591120
- DOI: 10.1097/TXD.0000000000001050
Hyponatremia Is Associated With Increased Mortality in Children on the Waiting List for Liver Transplantation
Abstract
Our aim was to determine whether hyponatremia is associated with waiting list or posttransplantation mortality in children having liver transplantation (LT).
Methods: A retrospective analysis of the united network for organ sharing/organ procurement transplantation network database on pediatric LT performed between 1988 and 2016 was conducted. Hyponatremia was defined as a serum sodium of 130 mEq/L or below. Subjects were divided into 2 age groups: I (0-6 y old) and II (7-18 y old). Patient survival before and after LT, as well as graft survival, were compared in patients with and without hyponatremia. Multivariable Cox proportional hazards models were constructed for perioperative mortality.
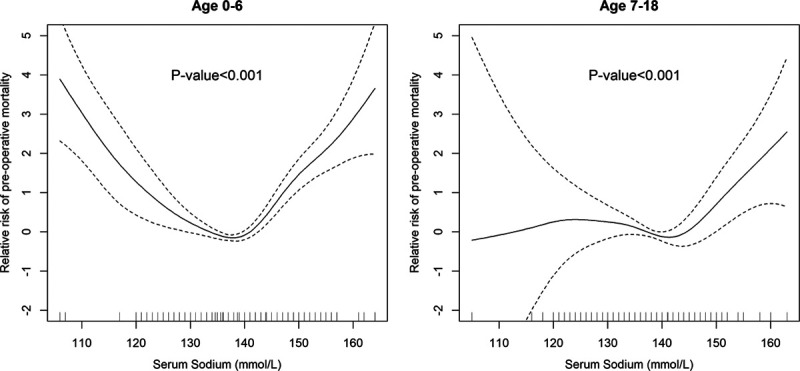
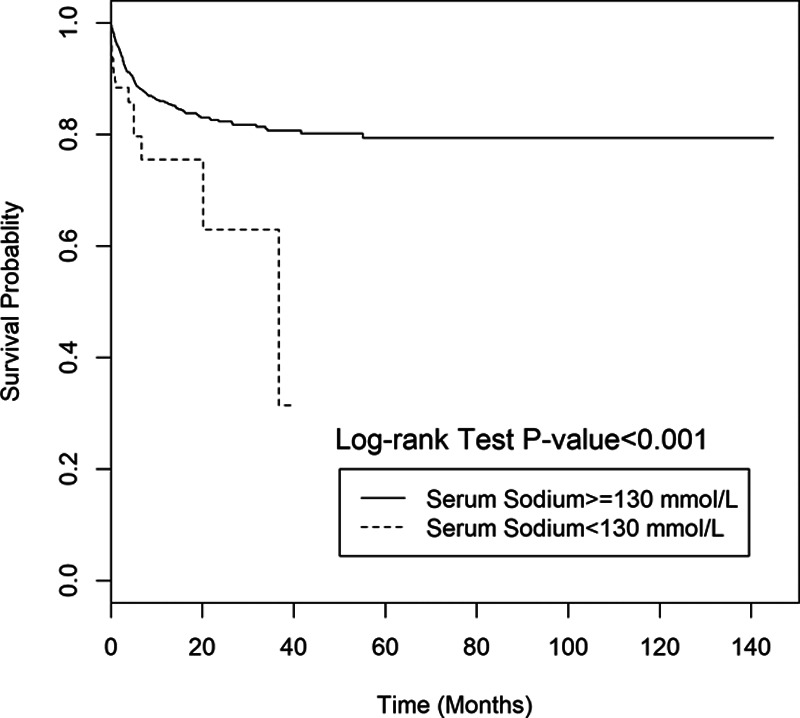
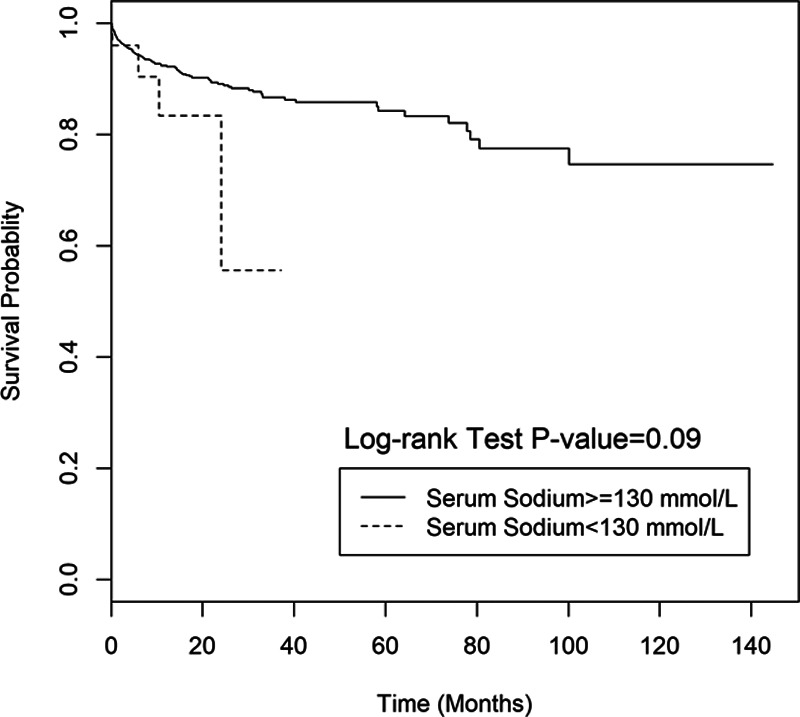
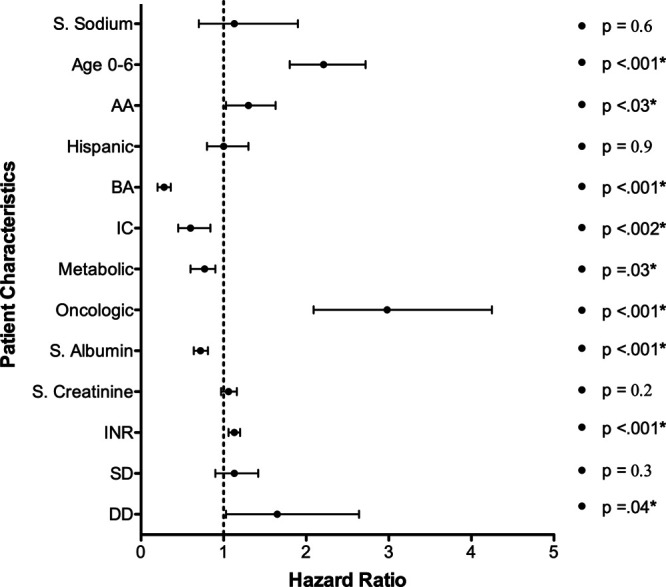
Results: Data from 6606 children were available for analysis of waiting list mortality, and 4478 for postoperative mortality. The prevalence of hyponatremia at the time of registration was 2.8% and 3.7% at the time of LT. Waiting list mortality in patients with hyponatremia was significantly higher in group I (P < 0.001) but not in group II (P = 0.09). In group I, the relative risk of mortality adjusted to pediatric end-stage liver disease score was significantly associated with hyponatremia (P < 0.001). A sodium level below 130 mEq/L (hazard ration [HR] = 1.7), younger age (group I) (HR = 2.01), and need for dialysis (HR = 2.3) were independent predictors for increased waiting list mortality. There was no difference in overall postoperative patient or graft survival related to hyponatremia.
Conclusions: Hyponatremia is associated with increased waiting list mortality for pediatric LT candidates, particularly in younger children. Future studies examining incorporation of age-specific serum sodium levels into organ allocation policies in children seems warranted based on our findings.
Copyright © 2020 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures

Similar articles
-
Serum sodium and survival benefit of liver transplantation.Liver Transpl. 2015 Mar;21(3):308-13. doi: 10.1002/lt.24063. Epub 2015 Feb 10. Liver Transpl. 2015. PMID: 25504743 Free PMC article.
-
Effect of the pretransplant serum sodium concentration on outcomes following liver transplantation.Liver Transpl. 2014 Jun;20(6):687-97. doi: 10.1002/lt.23860. Liver Transpl. 2014. PMID: 24616214 Free PMC article.
-
Extreme hyponatremia as a risk factor for early mortality after liver transplantation in the MELD-sodium era.Transpl Int. 2021 Dec;34(12):2856-2868. doi: 10.1111/tri.14123. Epub 2021 Oct 7. Transpl Int. 2021. PMID: 34580929 Free PMC article.
-
Intraoperative hyponatremia is an independent predictor of one-year mortality after liver transplantation.Sci Rep. 2018 Dec 21;8(1):18023. doi: 10.1038/s41598-018-37006-7. Sci Rep. 2018. PMID: 30575797 Free PMC article.
-
Hyponatremia and Liver Transplantation: A Narrative Review.J Cardiothorac Vasc Anesth. 2022 May;36(5):1458-1466. doi: 10.1053/j.jvca.2021.05.027. Epub 2021 May 23. J Cardiothorac Vasc Anesth. 2022. PMID: 34144870 Review.
Cited by
-
Clinical Implications, Evaluation, and Management of Hyponatremia in Cirrhosis.J Clin Exp Hepatol. 2022 Mar-Apr;12(2):575-594. doi: 10.1016/j.jceh.2021.09.008. Epub 2021 Sep 16. J Clin Exp Hepatol. 2022. PMID: 35535075 Free PMC article. Review.
-
Prevalence and risk factors of hyponatremia in hospitalized critically ill children: an observational study.Sudan J Paediatr. 2024;24(1):49-55. doi: 10.24911/SJP.106-1672832695. Sudan J Paediatr. 2024. PMID: 38952624 Free PMC article.
-
Accumulation of Postoperative Unexpected Events Assessed by the Comprehensive Complication Index® as Prognostic Outcome Parameters for Kasai Procedure.Children (Basel). 2022 Oct 20;9(10):1590. doi: 10.3390/children9101590. Children (Basel). 2022. PMID: 36291526 Free PMC article.
References
-
- Ginès P, Cárdenas A, Arroyo V, et al. Management of cirrhosis and ascites. N Engl J Med. 2004; 350:1646–1654. doi:10.1056/NEJMra035021 - PubMed
-
- Ginès P, Guevara M. Hyponatremia in cirrhosis: pathogenesis, clinical significance, and management. Hepatology. 2008; 48:1002–1010. doi:10.1002/hep.22418 - PubMed
-
- Martín-Llahí M, Guevara M, Ginès P. Hyponatremia in cirrhosis: clinical features and management. Gastroenterol Clin Biol. 2006; 30:1144–1151. doi:10.1016/S0399-8320(06)73492-3 - PubMed
-
- Angeli P, Wong F, Watson H, et al. ; CAPPS Investigators; CAPPS Investigators. Hyponatremia in cirrhosis: results of a patient population survey. Hepatology. 2006; 44:1535–1542. doi:10.1002/hep.21412 - PubMed
-
- Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000; 342:1581–1589. doi:10.1056/NEJM200005253422107 - PubMed
LinkOut - more resources
Full Text Sources
