

Deep-learning-based real-time prediction of acute kidney injury outperforms human predictive performance
- PMID: 33134556
- PMCID: PMC7588492
- DOI: 10.1038/s41746-020-00346-8
Deep-learning-based real-time prediction of acute kidney injury outperforms human predictive performance
Abstract
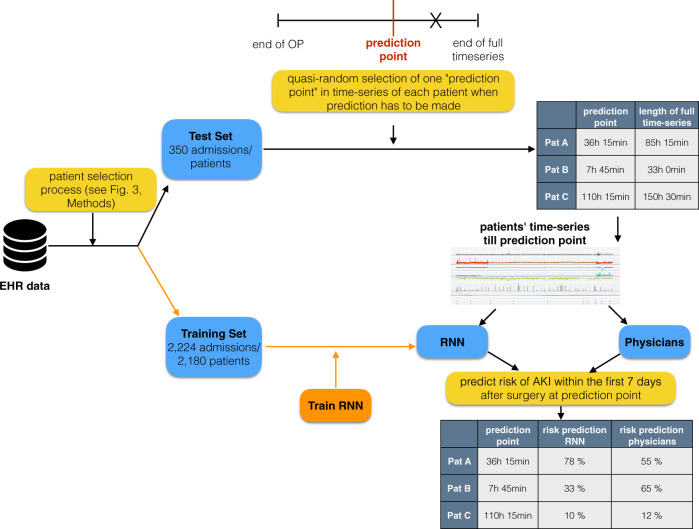
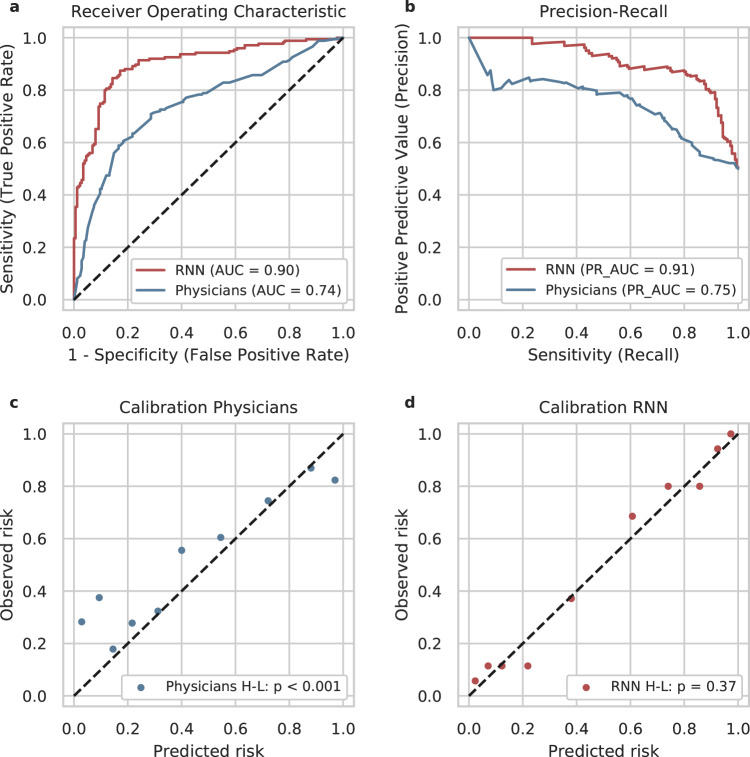
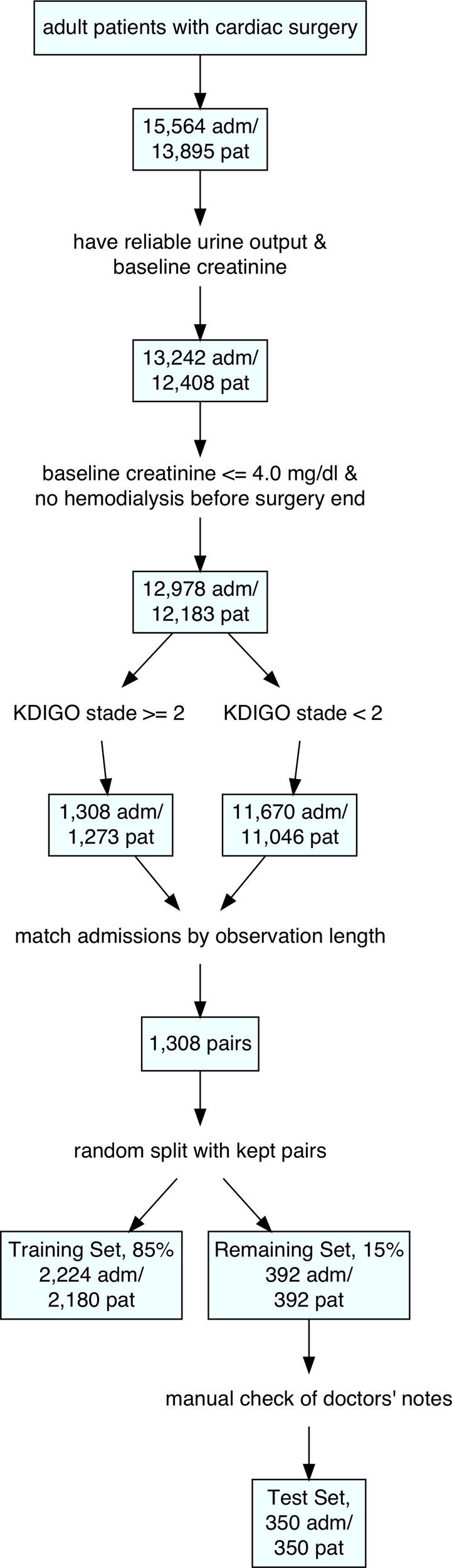
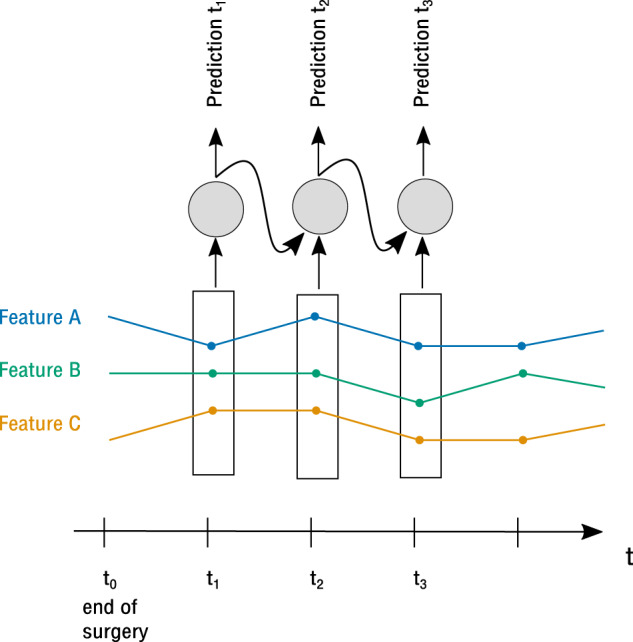
Acute kidney injury (AKI) is a major complication after cardiothoracic surgery. Early prediction of AKI could prompt preventive measures, but is challenging in the clinical routine. One important reason is that the amount of postoperative data is too massive and too high-dimensional to be effectively processed by the human operator. We therefore sought to develop a deep-learning-based algorithm that is able to predict postoperative AKI prior to the onset of symptoms and complications. Based on 96 routinely collected parameters we built a recurrent neural network (RNN) for real-time prediction of AKI after cardiothoracic surgery. From the data of 15,564 admissions we constructed a balanced training set (2224 admissions) for the development of the RNN. The model was then evaluated on an independent test set (350 admissions) and yielded an area under curve (AUC) (95% confidence interval) of 0.893 (0.862-0.924). We compared the performance of our model against that of experienced clinicians. The RNN significantly outperformed clinicians (AUC = 0.901 vs. 0.745, p < 0.001) and was overall well calibrated. This was not the case for the physicians, who systematically underestimated the risk (p < 0.001). In conclusion, the RNN was superior to physicians in the prediction of AKI after cardiothoracic surgery. It could potentially be integrated into hospitals' electronic health records for real-time patient monitoring and may help to detect early AKI and hence modify the treatment in perioperative care.
Keywords: Diagnosis; Preventive medicine.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsA.M. declares the receipt of consulting and lecturing fees from Medtronic GmbH and Edwards Lifesciences Services GmbH, and consulting fees from Pfizer. C.E. declares ownership of shares in codiag AG. F.S. declares the receipt of honoraria, consultancy fees or travel support from Medtronic GmbH, Biotronik SE & Co., Abbott GmbH & Co. KG, Sanofi S.A., Cardiorentis AG, Novartis Pharma GmbH. J.K. declares the receipt of lecturing fees from, Boston Scientific, LSI Solutions, Edwards, Medtronic, Abbott, Ascyrus Medical GmbH. V.F. declares (institutional) financial activities with Medtronic, Biotronik, Abbott, Boston, Edwards, Berlin Heart, Novartis, Jotec, Zurich Heart in relation to Educational Grants, honoraria, consultancy, research & study funds, fees for travel support. All other authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
