

Feasibility Case Study for Treating a Patient with Sensory Ataxia Following a Stroke with Kinesthetic Illusion Induced by Visual Stimulation
- PMID: 33134593
- PMCID: PMC7591318
- DOI: 10.2490/prm.20200025
Feasibility Case Study for Treating a Patient with Sensory Ataxia Following a Stroke with Kinesthetic Illusion Induced by Visual Stimulation
Abstract
Background: Sensory ataxia is a disorder of movement coordination caused by sensory deficits, especially in kinesthetic perception. Visual stimulus-induced kinesthetic illusion (KINVIS) is a method used to provide vivid kinesthetic perception without peripheral sensory input by using a video showing pre-recorded limb movements while the actual limb remains stationary. We examined the effects of KINVIS intervention in a patient with sensory ataxia.
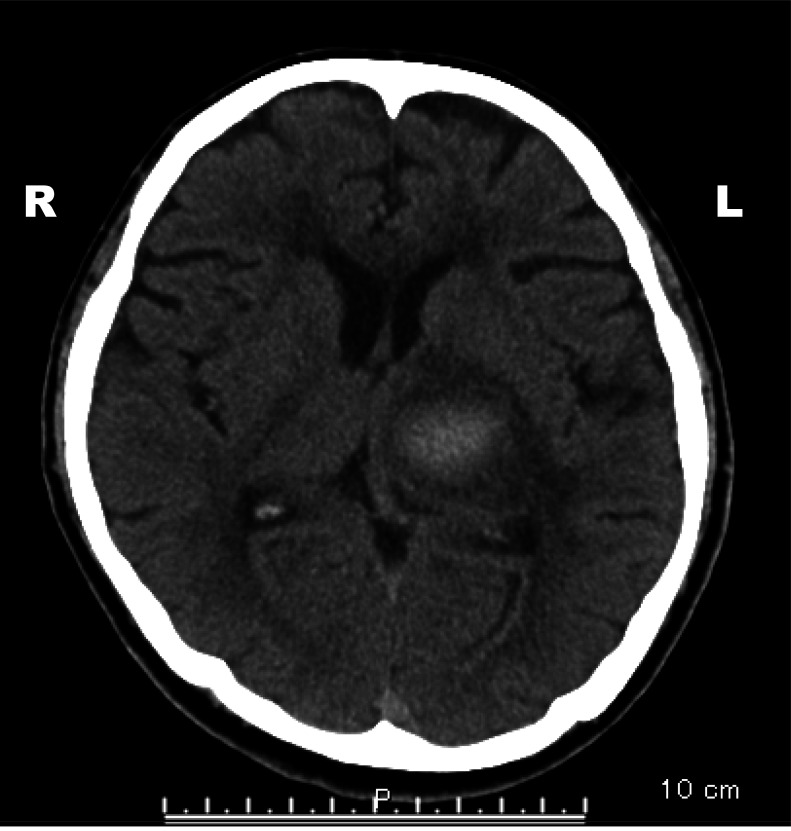
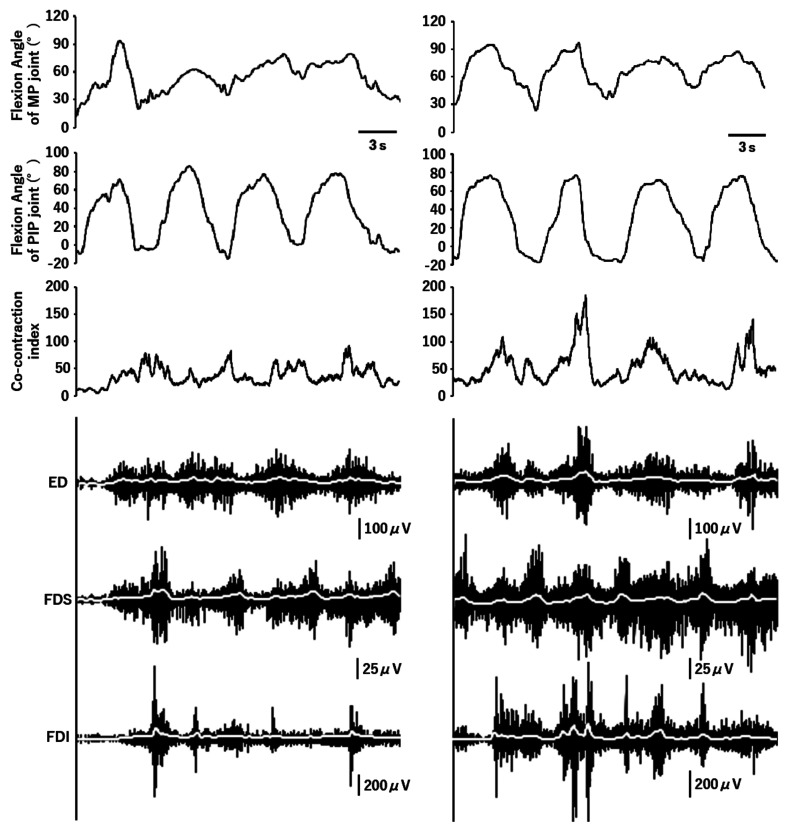
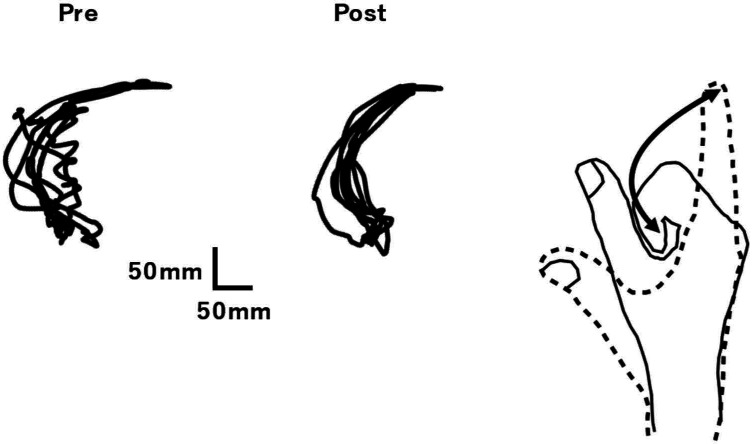
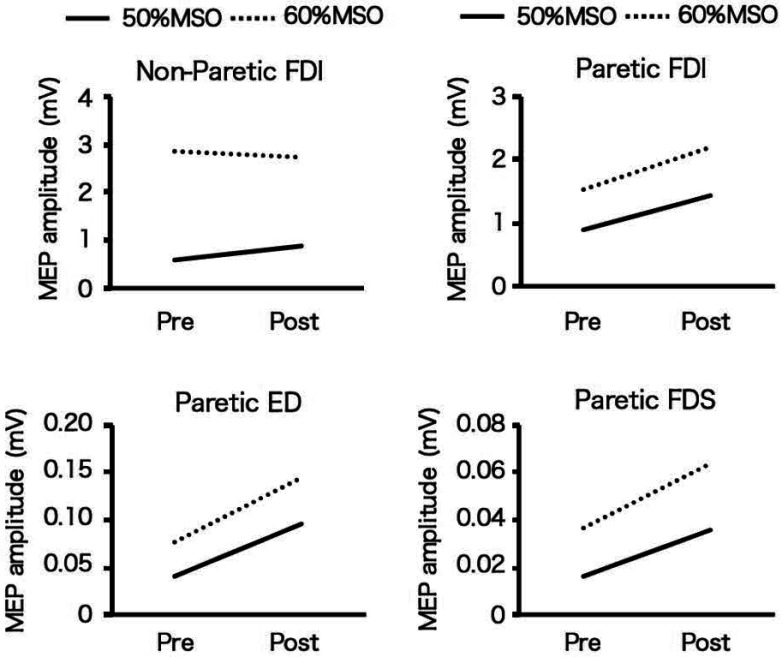
Case: The patient was a 59-year-old man with a severe proprioceptive deficit caused by left thalamic hemorrhage. During KINVIS intervention, a computer screen displayed a pre-recorded mirror image video of the patient's unaffected hand performing flexion-extension movements as if it were attached to the patient's affected forearm. Kinematics during the flexion-extension movements of the paretic hand were recorded before and after 20-min interventions. Transcranial magnetic stimulation was applied to the affected and non-affected hemispheres. The amplitude of the motor-evoked potential (MEP) at rest was recorded for the muscles of both hands. After the intervention, the total trajectory length and the rectangular area bounding the trajectory of the index fingertip decreased. The MEP amplitude of the paretic hand increased, whereas the MEP amplitude of the non-paretic hand was unchanged.
Discussion: The changes in kinematics after the intervention suggested that KINVIS therapy may be a useful new intervention for sensory ataxia, a condition for which few effective treatments are currently available. Studies in larger numbers of patients are needed to clarify the mechanisms underlying this therapeutic effect.
Keywords: body ownership; kinesthetic illusion; sensory ataxia; stroke; transcranial magnetic stimulation.
©2020 The Japanese Association of Rehabilitation Medicine.
Conflict of interest statement
CONFLICTS OF INTEREST: FK is the founding scientist of Connect Inc., a commercial company set up in October 2018 for the development of rehabilitation devices. This company does not have any relationship with the device or setup used in the present study. FK received license fees from Inter Reha Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Influence of Visual Stimulation-Induced Passive Reproduction of Motor Images in the Brain on Motor Paralysis After Stroke.Front Hum Neurosci. 2021 Jun 22;15:674139. doi: 10.3389/fnhum.2021.674139. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34239429 Free PMC article.
-
Kinesthetic illusion induced by visual stimulation influences sensorimotor event-related desynchronization in stroke patients with severe upper-limb paralysis: A pilot study.Restor Neurol Neurosci. 2020;38(6):455-465. doi: 10.3233/RNN-201030. Restor Neurol Neurosci. 2020. PMID: 33325415
-
Event-related desynchronization possibly discriminates the kinesthetic illusion induced by visual stimulation from movement observation.Exp Brain Res. 2019 Dec;237(12):3233-3240. doi: 10.1007/s00221-019-05665-1. Epub 2019 Oct 19. Exp Brain Res. 2019. PMID: 31630226
-
The association of motor imagery and kinesthetic illusion prolongs the effect of transcranial direct current stimulation on corticospinal tract excitability.J Neuroeng Rehabil. 2016 Apr 15;13:36. doi: 10.1186/s12984-016-0143-8. J Neuroeng Rehabil. 2016. PMID: 27079199 Free PMC article.
-
Sensing limb movements in the motor cortex: how humans sense limb movement.Neuroscientist. 2004 Feb;10(1):73-82. doi: 10.1177/1073858403259628. Neuroscientist. 2004. PMID: 14987450 Review.
Cited by
-
Model-Based Analyses for the Causal Relationship Between Post-stroke Impairments and Functional Brain Connectivity Regarding the Effects of Kinesthetic Illusion Therapy Combined With Conventional Exercise.Front Syst Neurosci. 2022 Jan 10;15:804263. doi: 10.3389/fnsys.2021.804263. eCollection 2021. Front Syst Neurosci. 2022. PMID: 35173590 Free PMC article.
-
Influence of Visual Stimulation-Induced Passive Reproduction of Motor Images in the Brain on Motor Paralysis After Stroke.Front Hum Neurosci. 2021 Jun 22;15:674139. doi: 10.3389/fnhum.2021.674139. eCollection 2021. Front Hum Neurosci. 2021. PMID: 34239429 Free PMC article.
-
Relationship between resting-state functional connectivity and change in motor function after motor imagery intervention in patients with stroke: a scoping review.J Neuroeng Rehabil. 2023 Nov 18;20(1):159. doi: 10.1186/s12984-023-01282-w. J Neuroeng Rehabil. 2023. PMID: 37980496 Free PMC article.