

The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis
- PMID: 33134905
- PMCID: PMC7584493
- DOI: 10.1016/j.eclinm.2020.100603
The potential impact of the COVID-19 pandemic on the tuberculosis epidemic a modelling analysis
Abstract
Background: Routine services for tuberculosis (TB) are being disrupted by stringent lockdowns against the novel SARS-CoV-2 virus. We sought to estimate the potential long-term epidemiological impact of such disruptions on TB burden in high-burden countries, and how this negative impact could be mitigated.
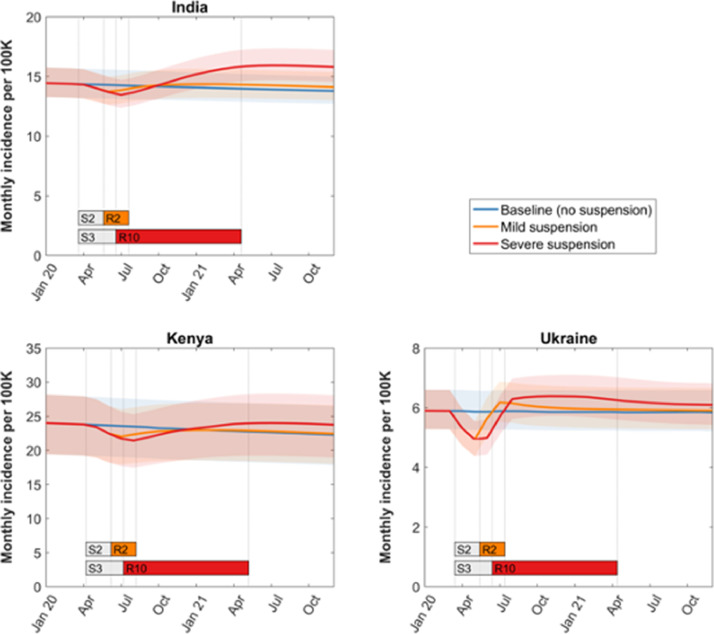
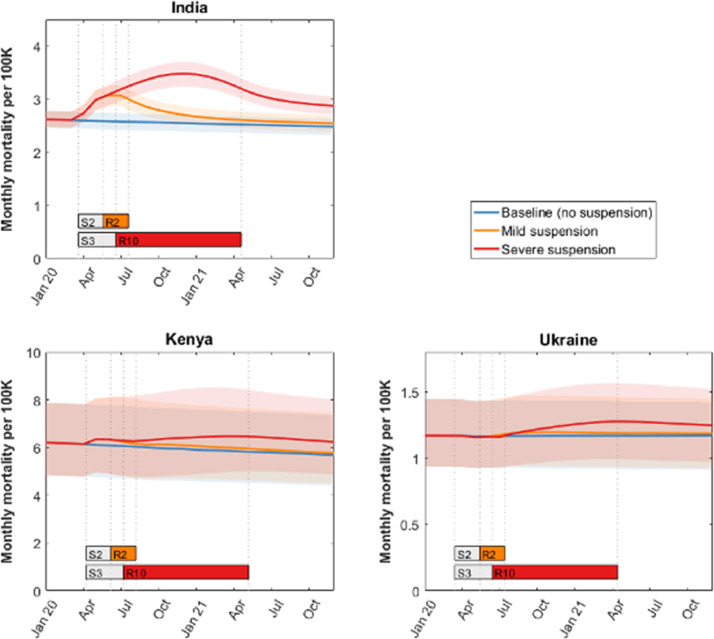
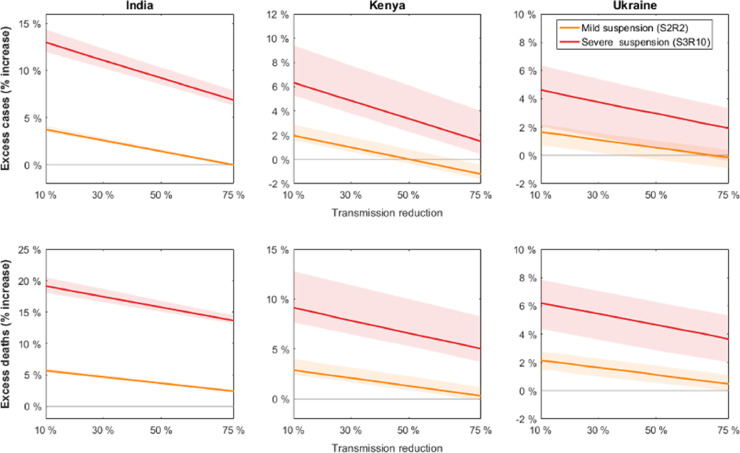
Methods: We adapted mathematical models of TB transmission in three high-burden countries (India, Kenya and Ukraine) to incorporate lockdown-associated disruptions in the TB care cascade. The anticipated level of disruption reflected consensus from a rapid expert consultation. We modelled the impact of these disruptions on TB incidence and mortality over the next five years, and also considered potential interventions to curtail this impact.
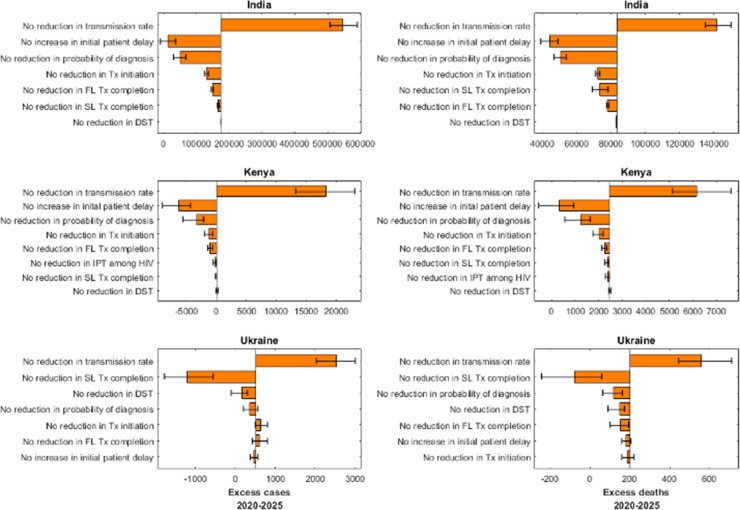
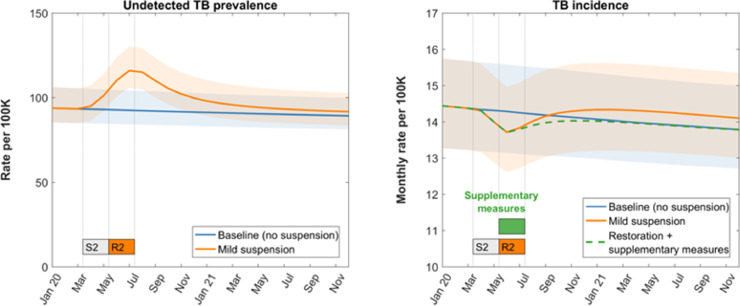
Findings: Even temporary disruptions can cause long-term increases in TB incidence and mortality. If lockdown-related disruptions cause a temporary 50% reduction in TB transmission, we estimated that a 3-month suspension of TB services, followed by 10 months to restore to normal, would cause, over the next 5 years, an additional 1⋅19 million TB cases (Crl 1⋅06-1⋅33) and 361,000 TB deaths (CrI 333-394 thousand) in India, 24,700 (16,100-44,700) TB cases and 12,500 deaths (8.8-17.8 thousand) in Kenya, and 4,350 (826-6,540) cases and 1,340 deaths (815-1,980) in Ukraine. The principal driver of these adverse impacts is the accumulation of undetected TB during a lockdown. We demonstrate how long term increases in TB burden could be averted in the short term through supplementary "catch-up" TB case detection and treatment, once restrictions are eased.
Interpretation: Lockdown-related disruptions can cause long-lasting increases in TB burden, but these negative effects can be mitigated with rapid restoration of TB services, and targeted interventions that are implemented as soon as restrictions are lifted.
Funding: USAID and Stop TB Partnership.
Keywords: Covid-19; Epidemiology; Mathematical modellingabstract; Tuberculosis.
© 2020 The Authors.
Conflict of interest statement
SA is employed by USAID and SAN, AM, EM, and SS are employed by the Stop TB Partnership. The other authors declare no conflicts of interest.
Figures
References
-
- Flaxman S., Mishra S., Gandy A. Estimating the number of infections and the impact of non-pharmaceutical interventions on COVID-19 in 11 European countries. Imp Coll Lond. 2020
LinkOut - more resources
Full Text Sources
Miscellaneous
