

Rationale and Strategies for Development of an Optimal Bundle of Management for Cardiac Arrest
- PMID: 33134932
- PMCID: PMC7566870
- DOI: 10.1097/CCE.0000000000000214
Rationale and Strategies for Development of an Optimal Bundle of Management for Cardiac Arrest
Abstract
Objectives: To construct a highly detailed yet practical, attainable roadmap for enhancing the likelihood of neurologically intact survival following sudden cardiac arrest.
Design setting and patients: Population-based outcomes following out-of-hospital cardiac arrest were collated for 10 U.S. counties in Alaska, California, Florida, Ohio, Minnesota, Utah, and Washington. The 10 identified emergency medical services systems were those that had recently reported significant improvements in neurologically intact survival after introducing a more comprehensive approach involving citizens, hospitals, and evolving strategies for incorporating technology-based, highly choreographed care and training. Detailed inventories of in-common elements were collated from the ten 9-1-1 agencies and assimilated. For reference, combined averaged outcomes for out-of-hospital cardiac arrest occurring January 1, 2017, to February 28, 2018, were compared with concurrent U.S. outcomes reported by the well-established Cardiac Arrest Registry to Enhance Survival.
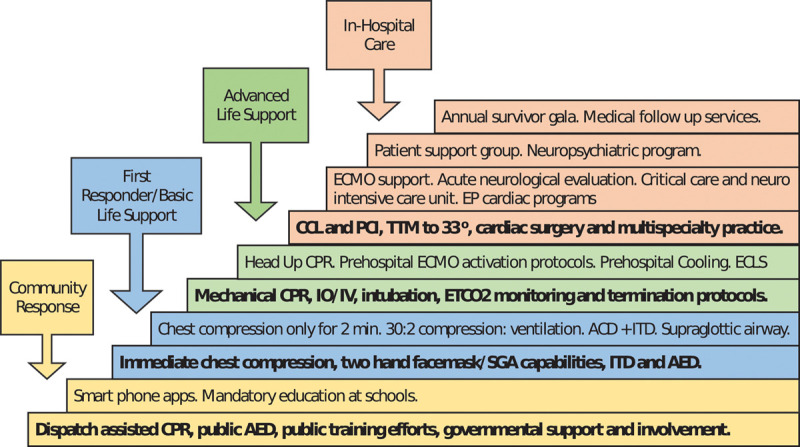
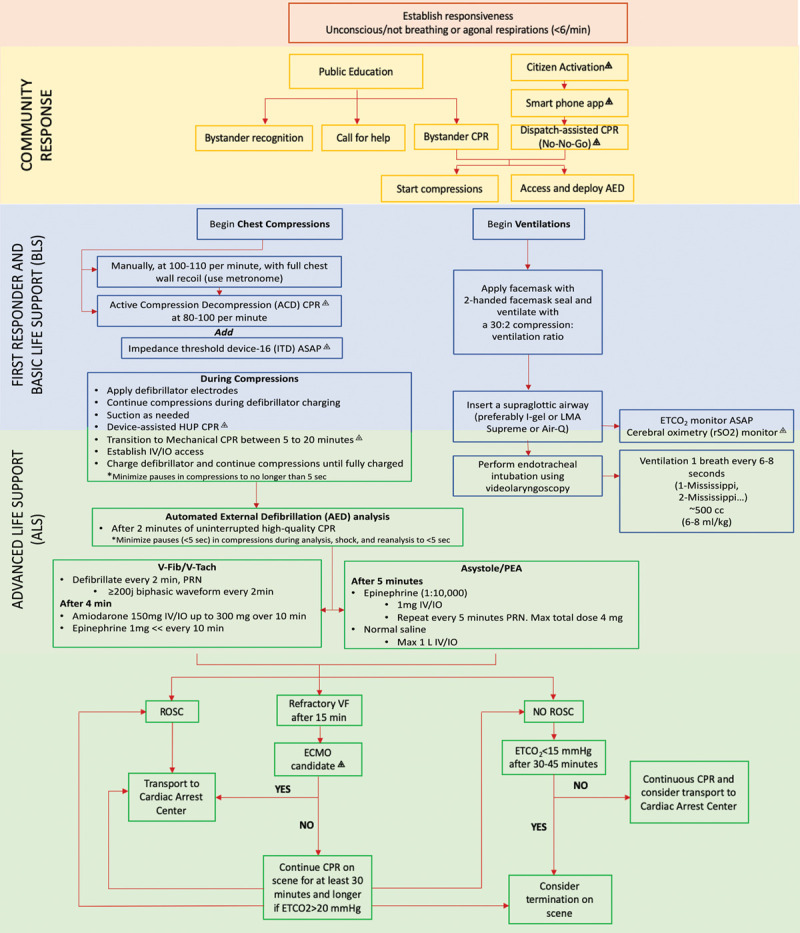
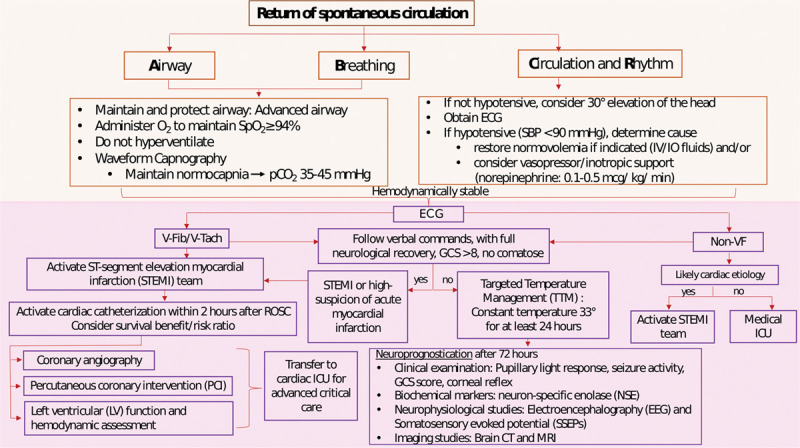
Interventions: Most commonly, interventions and components from the ten 9-1-1 systems consistently included extensive public cardiopulmonary resuscitation training, 9-1-1 system-connected smart phone applications, expedited dispatcher procedures, cardiopulmonary resuscitation quality monitoring, mechanical cardiopulmonary resuscitation, devices for enhancing negative intrathoracic pressure regulation, extracorporeal membrane oxygenation protocols, body temperature management procedures, rapid cardiac angiography, and intensive involvement of medical directors, operational and quality assurance officers, and training staff.
Measurements and main results: Compared with Cardiac Arrest Registry to Enhance Survival (n = 78,704), the cohorts from the 10 emergency medical services agencies examined (n = 2,911) demonstrated significantly increased likelihoods of return of spontaneous circulation (mean 37.4% vs 31.5%; p < 0.001) and neurologically favorable hospital discharge, particularly after witnessed collapses involving bystander cardiopulmonary resuscitation and shockable cardiac rhythms (mean 10.7% vs 8.4%; p < 0.001; and 41.6% vs 29.2%; p < 0.001, respectively).
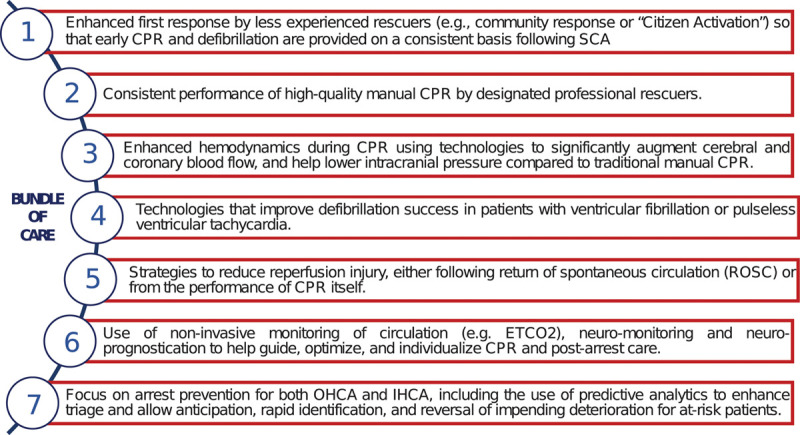
Conclusions: The likelihood of neurologically favorable survival following out-of-hospital cardiac arrest can improve substantially in communities that conscientiously and meticulously introduce a well-sequenced, highly choreographed, system-wide portfolio of both traditional and nonconventional approaches to training, technologies, and physiologic management. The commonalities found in the analyzed systems create a compelling case that other communities can also improve out-of-hospital cardiac arrest outcomes significantly by conscientiously exploring and adopting similar bundles of system organization and care.
Keywords: bundle of care; cardiac arrest; cardiopulmonary resuscitation; emergency medical services; resuscitation centers; sudden cardiac death survival.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Lurie who is a coinventor of multiple CPR devices and founder of Advanced CPR Solutions LLC, that develops novel resuscitation technologies. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Benjamin EJ, Muntner P, Alonso A, et al. ; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation. 2019; 139:e56–e528 - PubMed
-
- Abrams HC, McNally B, Ong M, et al. . A composite model of survival from out-of-hospital cardiac arrest using the cardiac arrest registry to enhance survival (CARES). Resuscitation. 2013; 84:1093–1098 - PubMed
-
- Perkins GD, Neumar R, Monsieurs KG, et al. ; International Liaison Committee on Resuscitation. The international liaison committee on resuscitation-review of the last 25 years and vision for the future. Resuscitation. 2017; 121:104–116 - PubMed
-
- Soar J, Donnino MW, Maconochie I, et al. ; ILCOR Collaborators. 2018 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations summary. Circulation. 2018; 138:e714–e730 - PubMed
LinkOut - more resources
Full Text Sources
