

Off-target effects of sodium-glucose co-transporter 2 blockers: empagliflozin does not inhibit Na+/H+ exchanger-1 or lower [Na+]i in the heart
- PMID: 33135077
- PMCID: PMC8683707
- DOI: 10.1093/cvr/cvaa323
Off-target effects of sodium-glucose co-transporter 2 blockers: empagliflozin does not inhibit Na+/H+ exchanger-1 or lower [Na+]i in the heart
Abstract
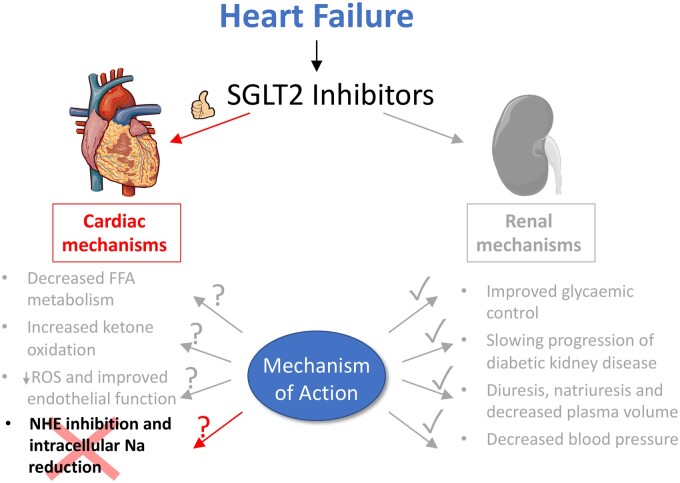
Aims: Emipagliflozin (EMPA) is a potent inhibitor of the renal sodium-glucose co-transporter 2 (SGLT2) and an effective treatment for type-2 diabetes. In patients with diabetes and heart failure, EMPA has cardioprotective effects independent of improved glycaemic control, despite SGLT2 not being expressed in the heart. A number of non-canonical mechanisms have been proposed to explain these cardiac effects, most notably an inhibitory action on cardiac Na+/H+ exchanger 1 (NHE1), causing a reduction in intracellular [Na+] ([Na+]i). However, at resting intracellular pH (pHi), NHE1 activity is very low and its pharmacological inhibition is not expected to meaningfully alter steady-state [Na+]i. We re-evaluate this putative EMPA target by measuring cardiac NHE1 activity.
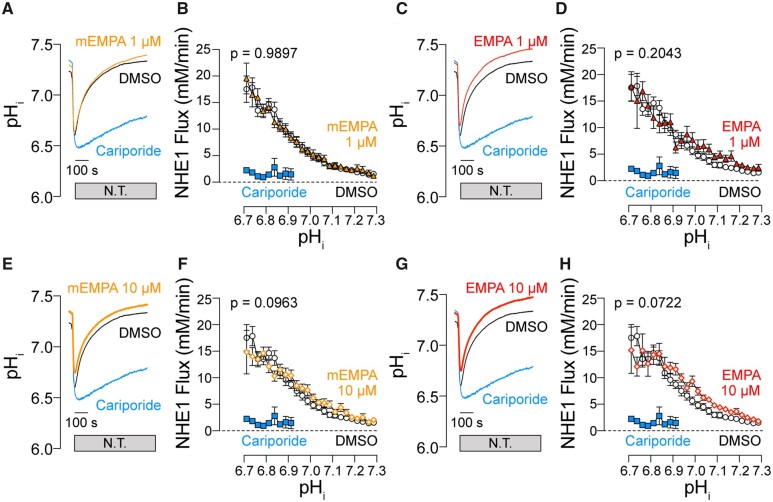
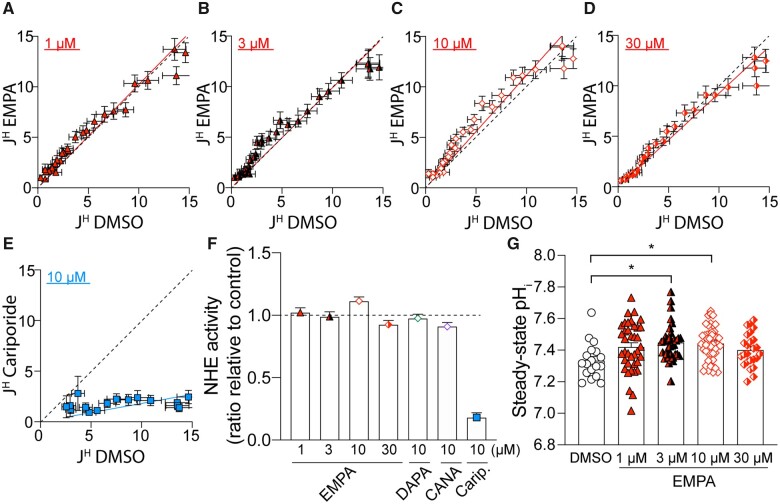
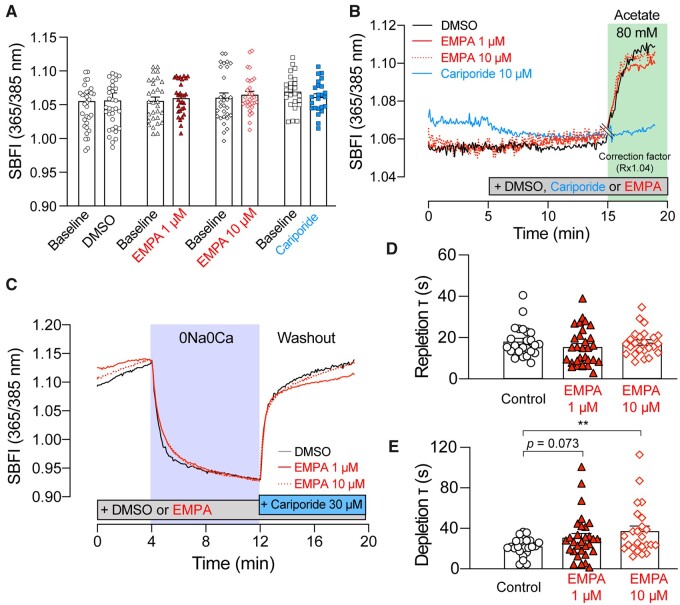
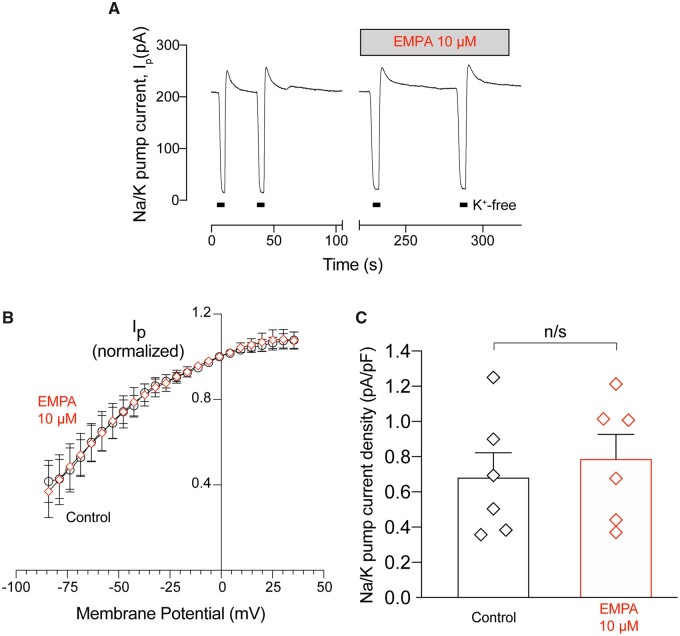
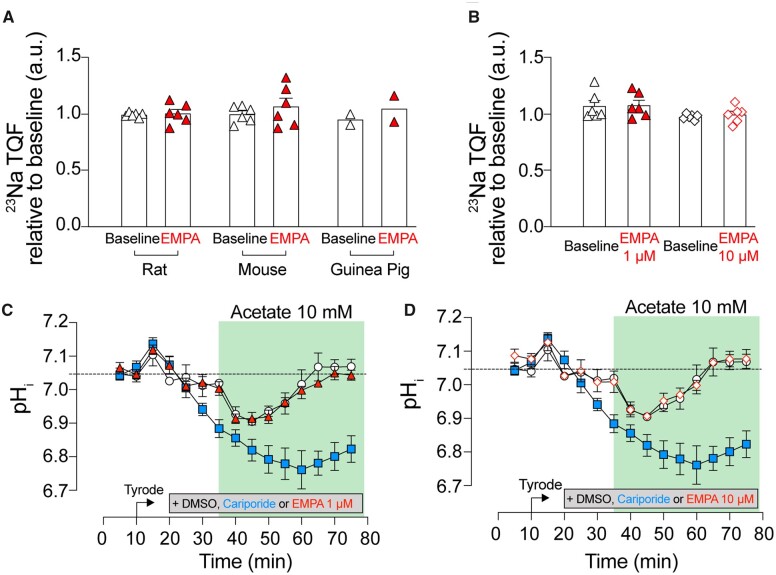
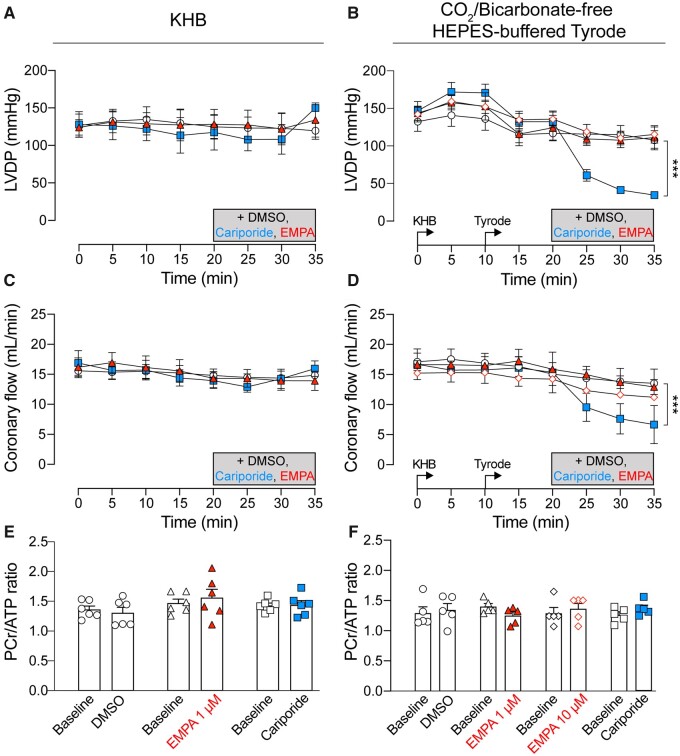
Methods and results: The effect of EMPA on NHE1 activity was tested in isolated rat ventricular cardiomyocytes from measurements of pHi recovery following an ammonium pre-pulse manoeuvre, using cSNARF1 fluorescence imaging. Whereas 10 µM cariporide produced near-complete inhibition, there was no evidence for NHE1 inhibition with EMPA treatment (1, 3, 10, or 30 µM). Intracellular acidification by acetate-superfusion evoked NHE1 activity and raised [Na+]i, reported by sodium binding benzofuran isophthalate (SBFI) fluorescence, but EMPA did not ablate this rise. EMPA (10 µM) also had no significant effect on the rate of cytoplasmic [Na+]i rise upon superfusion of Na+-depleted cells with Na+-containing buffers. In Langendorff-perfused mouse, rat and guinea pig hearts, EMPA did not affect [Na+]i at baseline nor pHi recovery following acute acidosis, as measured by 23Na triple quantum filtered NMR and 31P NMR, respectively.
Conclusions: Our findings indicate that cardiac NHE1 activity is not inhibited by EMPA (or other SGLT2i's) and EMPA has no effect on [Na+]i over a wide range of concentrations, including the therapeutic dose. Thus, the beneficial effects of SGLT2i's in failing hearts should not be interpreted in terms of actions on myocardial NHE1 or intracellular [Na+].
Keywords: Heart failure; Intracellular Na; NMR spectroscopy; Na/H exchanger-1; SGLT2 inhibitor.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Does the cardioprotective effect of Empagliflozin involve inhibition of the sodium-proton exchanger?Cardiovasc Res. 2021 Dec 17;117(14):2696-2698. doi: 10.1093/cvr/cvab137. Cardiovasc Res. 2021. PMID: 34021316 Free PMC article. No abstract available.
References
-
- Grempler R, Thomas L, Eckhardt M, Himmelsbach F, Sauer A, Sharp DE, Bakker RA, Mark M, Klein T, Eickelmann P.. Empagliflozin, a novel selective sodium glucose cotransporter-2 (SGLT-2) inhibitor: characterisation and comparison with other SGLT-2 inhibitors. Diabetes Obes Metab 2012;14:83–90. - PubMed
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE, EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015;373:2117–2128. - PubMed
-
- Yurista SR, Silljé HHW, Oberdorf-Maass SU, Schouten E-M, Pavez Giani MG, Hillebrands J-L, van Goor H, van Veldhuisen DJ, de Boer RA, Westenbrink BD.. Sodium-glucose co-transporter 2 inhibition with empagliflozin improves cardiac function in non-diabetic rats with left ventricular dysfunction after myocardial infarction. Eur J Heart Fail 2019;21:862–873. - PubMed
-
- Li C, Zhang J, Xue M, Li X, Han F, Liu X, Xu L, Lu Y, Cheng Y, Li T, Yu X, Sun B, Chen L.. SGLT2 inhibition with empagliflozin attenuates myocardial oxidative stress and fibrosis in diabetic mice heart. Cardiovasc Diabetol 2019;18:https://doi.org/10.1186/s12933-019-0816-2 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
