Expert-level segmentation using deep learning for volumetry of polycystic kidney and liver
- PMID: 33135401
- PMCID: PMC7606119
- DOI: 10.4111/icu.20200086
Expert-level segmentation using deep learning for volumetry of polycystic kidney and liver
Abstract
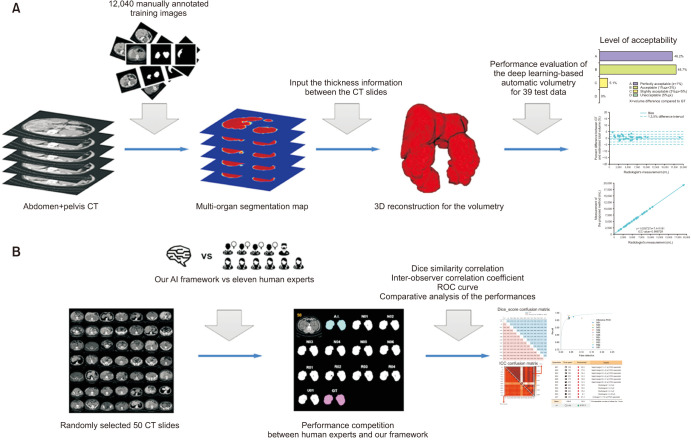
Purpose: Volumetry is used in polycystic kidney and liver diseases (PKLDs), including autosomal dominant polycystic kidney disease (ADPKD), to assess disease progression and drug efficiency. However, since no rapid and accurate method for volumetry has been developed, volumetry has not yet been established in clinical practice, hindering the development of therapies for PKLD. This study presents an artificial intelligence (AI)-based volumetry method for PKLD.
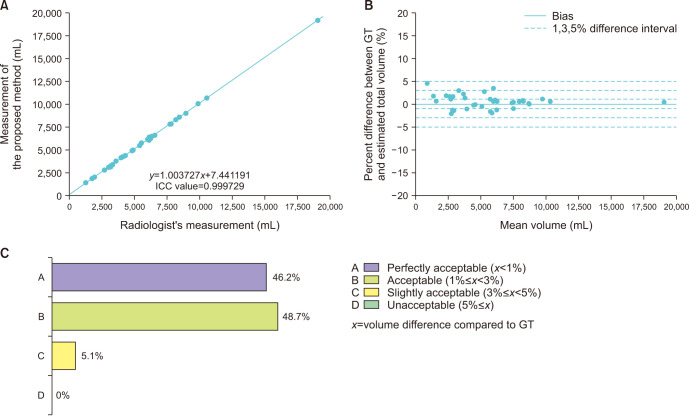
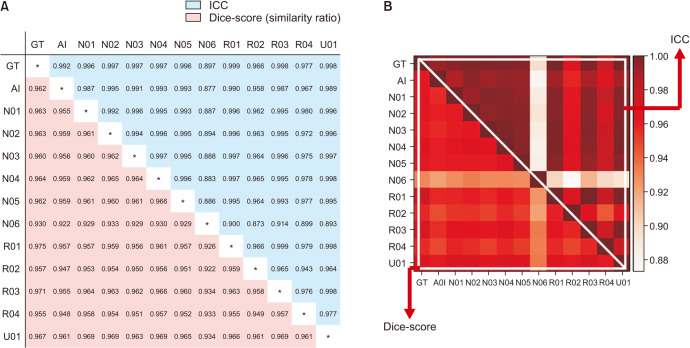
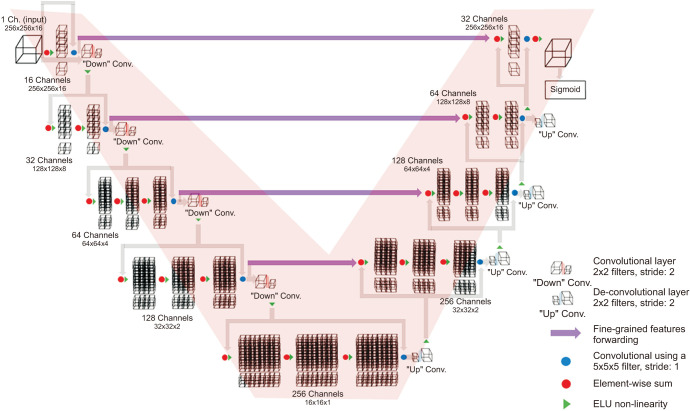
Materials and methods: The performance of AI was first evaluated in comparison with ground-truth (GT). We trained a V-net-based convolutional neural network on 175 ADPKD computed tomography (CT) segmentations, which served as the GT and were agreed upon by 3 experts using images from 214 patients analyzed with volumetry. The dice similarity coefficient (DSC), interobserver correlation coefficient (ICC), and Bland-Altman plots of 39 GT and AI segmentations in the validation set were compared. Next, the performance of AI on the segmentation of 50 random CT images was compared with that of 11 PKLD specialists based on the resulting DSC and ICC.
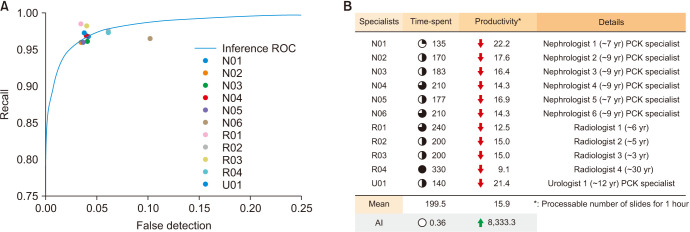
Results: The DSC and ICC of the AI were 0.961 and 0.999729, respectively. The error rate was within 3% for approximately 95% of the CT scans (error<1%, 46.2%; 1%≤error<3%, 48.7%). Compared with the specialists, AI showed moderate performance. Furthermore, an outlier in our results confirmed that even PKLD specialists can make mistakes in volumetry.
Conclusions: PKLD volumetry using AI was fast and accurate. AI performed comparably to human specialists, suggesting its use may be practical in clinical settings.
Keywords: Artificial intelligence; Polycystic kidney diseases; Tomography.
© The Korean Urological Association, 2020.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Harris PC. Autosomal dominant polycystic kidney disease: clues to pathogenesis. Hum Mol Genet. 1999;8:1861–1866. - PubMed
-
- Bae KT, Zhu F, Chapman AB, Torres VE, Grantham JJ, Guay-Woodford LM, et al. Magnetic resonance imaging evaluation of hepatic cysts in early autosomal-dominant polycystic kidney disease: the Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease cohort. Clin J Am Soc Nephrol. 2006;1:64–69. - PubMed
-
- Chauveau D, Fakhouri F, Grünfeld JP. Liver involvement in autosomal-dominant polycystic kidney disease: therapeutic dilemma. J Am Soc Nephrol. 2000;11:1767–1775. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous