

Slope-Correction Osteotomy with Lateral Extra-articular Tenodesis and Revision Anterior Cruciate Ligament Reconstruction Is Highly Effective in Treating High-Grade Anterior Knee Laxity
- PMID: 33135908
- PMCID: PMC7705640
- DOI: 10.1177/0363546520966327
Slope-Correction Osteotomy with Lateral Extra-articular Tenodesis and Revision Anterior Cruciate Ligament Reconstruction Is Highly Effective in Treating High-Grade Anterior Knee Laxity
Abstract
Background: Both an elevated posterior tibial slope (PTS) and high-grade anterior knee laxity are often present in patients who undergo revision anterior cruciate ligament (ACL) surgery, and these conditions are independent risk factors for ACL graft failure. Clinical data on slope-correction osteotomy combined with lateral extra-articular tenodesis (LET) do not yet exist.
Purpose: To evaluate the outcomes of patients undergoing revision ACL reconstruction (ACLR) and slope-correction osteotomy combined with LET.
Study design: Case series; Level of evidence, 4.
Methods: Between 2016 and 2018, we performed a 2-stage procedure: slope-correction osteotomy was performed first, and then revision ACLR in combination with LET was performed in 22 patients with ACLR failure and high-grade anterior knee laxity. Twenty patients (6 women and 14 men; mean age, 27.8 ± 8.6 years; range, 18-49 years) were evaluated, with a mean follow-up of 30.5 ± 9.3 months (range, 24-56 months), in this retrospective case series. Postoperative failure was defined as a side-to-side difference of ≥5 mm in the Rolimeter test and a pivot-shift grade of 2 or 3.
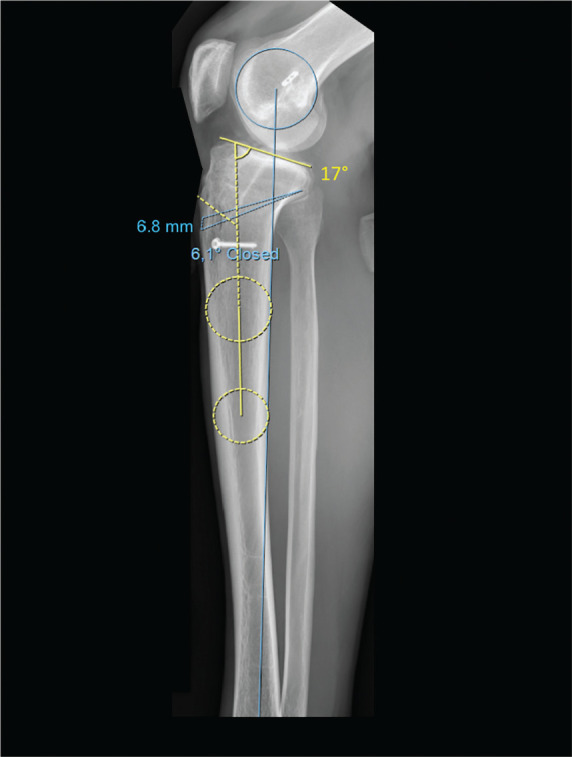
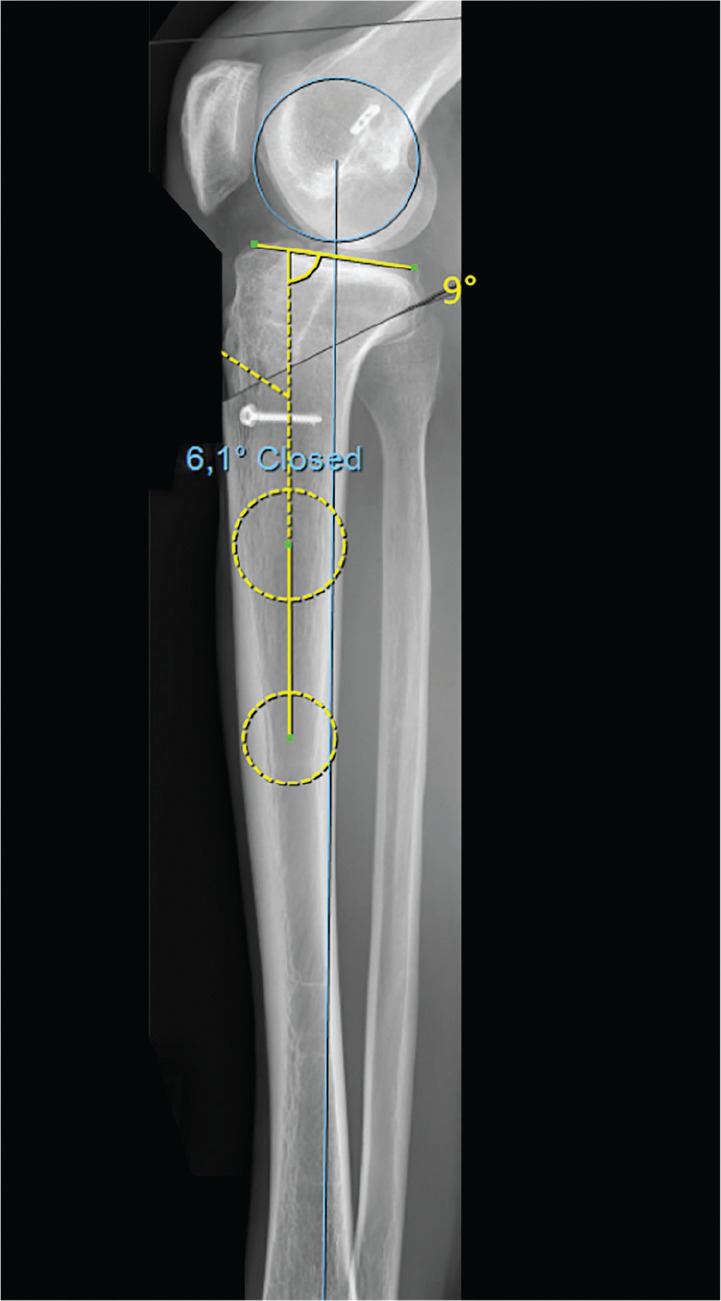
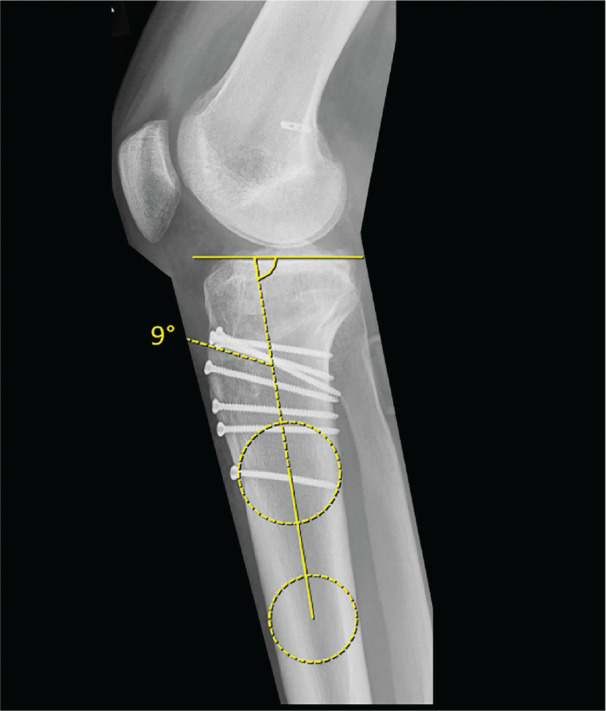
Results: The PTS decreased from 15.3° to 8.9°, the side-to-side difference decreased from 7.2 to 1.1 mm, and the pivot shift was no longer evident in any of the patients. No patients exhibited revision ACLR failure and all patients showed good to excellent postoperative functional scores (mean ± SD: visual analog scale, 0.5 ± 0.6; Tegner, 6.1 ± 0.9; Lysholm, 90.9 ± 6.4; Knee injury and Osteoarthritis Outcome Score [KOOS] Symptoms, 95.2 ± 8.4; KOOS Pain, 94.7 ± 5.2; KOOS Activities of Daily Living, 98.5 ± 3.2; KOOS Function in Sport and Recreation, 86.8 ± 12.4; and KOOS Quality of Life, 65.4 ± 14.9).
Conclusion: Slope-correction osteotomy in combination with LET is a safe and reliable procedure in patients with high-grade anterior knee laxity and a PTS of ≥12°. Normal knee joint stability was restored and good to excellent functional scores were achieved after a follow-up of at least 2 years.
Keywords: high-grade anterior knee instability; increased posterior tibial slope; revision anterior cruciate ligament reconstruction; slope-correction osteotomy.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: K.-H.F. received royalties and payment for educational support from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures


References
-
- Bernhardson AS, Aman ZS, Dornan GJ, et al. Tibial slope and its effect on force in anterior cruciate ligament grafts: anterior cruciate ligament force increases linearly as posterior tibial slope increases. Am J Sports Med. 2019;47(2):296-302. - PubMed
-
- Collins NJ, Prinsen CA, Christensen R, Bartels EM, Terwee CB, Roos EM. Knee injury and Osteoarthritis Outcome Score (KOOS): systematic review and meta-analysis of measurement properties. Osteoarthritis Cartilage. 2016;24(8):1317-1329. - PubMed
-
- Dejour H, Bonnin M. Tibial translation after anterior cruciate ligament rupture. Two radiological tests compared. J Bone Joint Surg Br. 1994;76(5):745-749. - PubMed
-
- Dejour D, La Barbera G, Pasqualotto S, et al. Sagittal plane corrections around the knee. J Knee Surg. 2017;30(8):736-745. - PubMed
-
- Dejour D, Saffarini M, Demey G, Baverel L. Tibial slope correction combined with second revision ACL produces good knee stability and prevents graft rupture. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):2846-2852. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
