

Effectiveness of Internet-Based Multicomponent Interventions for Patients and Health Care Professionals to Improve Clinical Outcomes in Type 2 Diabetes Evaluated Through the INDICA Study: Multiarm Cluster Randomized Controlled Trial
- PMID: 33136059
- PMCID: PMC7669446
- DOI: 10.2196/18922
Effectiveness of Internet-Based Multicomponent Interventions for Patients and Health Care Professionals to Improve Clinical Outcomes in Type 2 Diabetes Evaluated Through the INDICA Study: Multiarm Cluster Randomized Controlled Trial
Abstract
Background: Type 2 diabetes mellitus (T2DM) is a chronic disease in which health outcomes are related to decision making by patients and health care professionals.
Objective: This study aims to assess the effectiveness of internet-based multicomponent interventions to support decision making of all actors involved in the care of patients with T2DM in primary care.
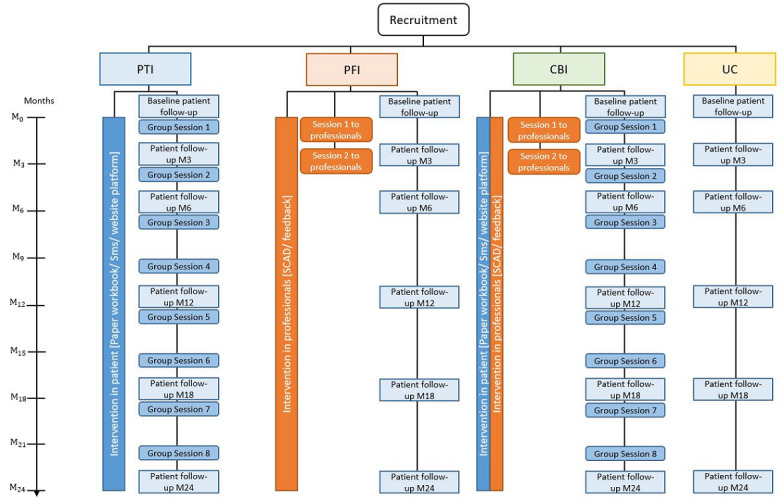
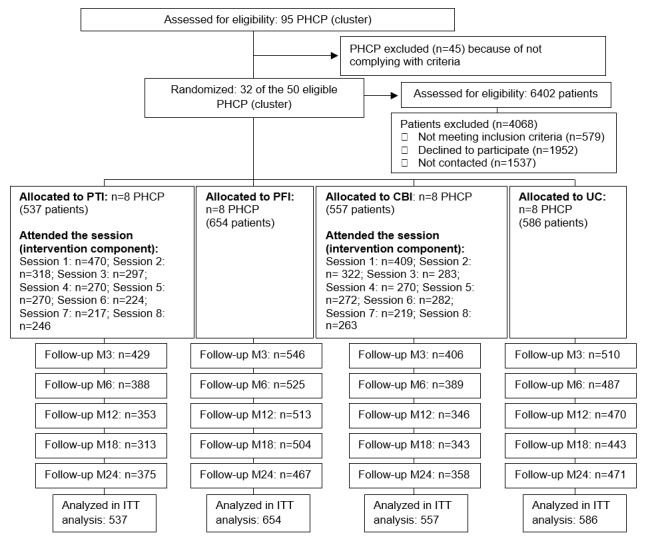
Methods: The INDICA study is an open, community-based, multicenter trial with random allocation to usual care or the intervention for patients, the intervention for health care professionals in primary care, or the combined intervention for both. In the intervention for patients, participants received an educational group program and were monitored and supported by logs, a web-based platform, and automated SMS. Those in the intervention for professionals also received an educational program, a decision support tool embedded in the electronic clinical record, and periodic feedback about patients' results. A total of 2334 people with T2DM, regardless of glycated hemoglobin (HbA1c) levels and without diabetes-related complications, were included. The primary end point was change in HbA1c level. The main analysis was performed using multilevel mixed models.
Results: For the overall sample, the intervention for patients attained a significant mean reduction in HbA1c levels of ‒0.27 (95% CI ‒0.45 to ‒0.10) at month 3 and ‒0.26 (95% CI ‒0.44 to ‒0.08) at month 6 compared with usual care, which remained marginally significant at month 12. A clinically relevant reduction in HbA1c level was observed in 35.6% (191/537) of patients in the intervention for patients and 26.0% (152/586) of those in usual care at month 12 (P=.006). In the combined intervention, HbA1c reduction was significant until month 18 (181/557, 32.6% vs 140/586, 23.9%; P=.009). Considering the subgroup of patients uncontrolled at baseline, all interventions produced significant reductions in HbA1c levels across the entire study period: ‒0.49 (95% CI ‒0.70 to ‒0.27) for the intervention for patients, ‒0.35 (95% CI ‒0.59 to ‒0.14) for the intervention for professionals, and ‒0.35 (95% CI ‒0.57 to ‒0.13) for the combined intervention. Differences in HbA1c for the area under the curve considering the entire period were significant for the intervention for patients and the combined intervention compared with usual care (P=.03 for both). Compared with usual care, the intervention for professionals and the combined intervention had significant longer-term reductions in systolic and diastolic blood pressure.
Conclusions: In uncontrolled patients, the intervention for patients at baseline provided clinically relevant and significant longer-term reductions of HbA1c levels. The intervention for professionals and combined intervention also improved the cardiovascular risk profile of patients.
Trial registration: ClinicalTrials.gov NCT01657227; https://clinicaltrials.gov/ct2/show/NCT01657227.
Keywords: behavior modification; eHealth; patients adherence; primary care; type 2 diabetes mellitus.
©Yolanda Ramallo-Fariña, Miguel Angel García-Bello, Lidia García-Pérez, Mauro Boronat, Ana M Wägner, Leticia Rodríguez-Rodríguez, Pedro de Pablos-Velasco, Ignacio Llorente Gómez de Segura, Himar González- Pacheco, Montserrat Carmona Rodríguez, Pedro Serrano-Aguilar, INDICA Team. Originally published in JMIR mHealth and uHealth (http://mhealth.jmir.org), 02.11.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Cabrera de León A, Rodríguez Pérez MC, Almeida González D, Domínguez Coello S, Aguirre Jaime A, Brito Díaz B, González Hernández A, Pérez Méndez LI, grupo CDC [Presentation of the 'CDC de Canarias' cohort: objectives, design and preliminary results] Rev Esp Salud Publica. 2008;82(5):519–34. doi: 10.1590/s1135-57272008000500007. https://www.mscbs.gob.es/biblioPublic/publicaciones/recursos_propios/res... - DOI - PubMed
-
- Lorenzo V, Boronat M, Saavedra P, Rufino M, Maceira B, Novoa FJ, Torres A. Disproportionately high incidence of diabetes-related end-stage renal disease in the Canary Islands. An analysis based on estimated population at risk. Nephrol Dial Transplant. 2010 Jul;25(7):2283–8. doi: 10.1093/ndt/gfp761. - DOI - PubMed
-
- Aragón-Sánchez J, García-Rojas A, Lázaro-Martínez JL, Quintana-Marrero Y, Maynar-Moliner M, Rabellino M, Hernández-Herrero MJ, Cabrera-Galván JJ. Epidemiology of diabetes-related lower extremity amputations in Gran Canaria, Canary Islands (Spain) Diabetes Res Clin Pract. 2009 Oct;86(1):e6–8. doi: 10.1016/j.diabres.2009.06.015. - DOI - PubMed
-
- Registro De Defunciones Según La Causa De Muerte. Instituto Nacional de Estadística, INE. 2015. [2020-10-01]. https://www.ine.es/jaxi/Datos.htm?path=/t15/p417/a2018/l0/&file=02001.px...
-
- Lopez-Bastida J, Boronat M, Moreno JO, Schurer W. Costs, outcomes and challenges for diabetes care in Spain. Global Health. 2013 May 1;9:17. doi: 10.1186/1744-8603-9-17. https://globalizationandhealth.biomedcentral.com/articles/10.1186/1744-8... - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
