

Lifestyle Intervention With or Without Lay Volunteers to Prevent Type 2 Diabetes in People With Impaired Fasting Glucose and/or Nondiabetic Hyperglycemia: A Randomized Clinical Trial
- PMID: 33136119
- PMCID: PMC7607494
- DOI: 10.1001/jamainternmed.2020.5938
Lifestyle Intervention With or Without Lay Volunteers to Prevent Type 2 Diabetes in People With Impaired Fasting Glucose and/or Nondiabetic Hyperglycemia: A Randomized Clinical Trial
Abstract
Importance: Nearly half of the older adult population has diabetes or a high-risk intermediate glycemic category, but we still lack trial evidence for effective type 2 diabetes prevention interventions in most of the current high-risk glycemic categories.
Objective: To determine whether a group-based lifestyle intervention (with or without trained volunteers with type 2 diabetes) reduced the risk of progression to type 2 diabetes in populations with a high-risk glycemic category.
Design, setting, and participants: The Norfolk Diabetes Prevention Study was a parallel, 3-arm, group-based, randomized clinical trial conducted with up to 46 months of follow-up from August 2011 to January 2019 at 135 primary care practices and 8 intervention sites in the East of England. We identified 141 973 people at increased risk of type 2 diabetes, screened 12 778 (9.0%), and randomized those with a high-risk glycemic category, which was either an elevated fasting plasma glucose level alone (≥110 and <126 mg/dL [to convert to millimoles per liter, multiply by 0.0555]) or an elevated glycated hemoglobin level (≥6.0% to <6.5%; nondiabetic hyperglycemia) with an elevated fasting plasma glucose level (≥100 to <110 mg/dL).
Interventions: A control arm receiving usual care (CON), a theory-based lifestyle intervention arm of 6 core and up to 15 maintenance sessions (INT), or the same intervention with support from diabetes prevention mentors, trained volunteers with type 2 diabetes (INT-DPM).
Main outcomes and measures: Type 2 diabetes incidence between arms.
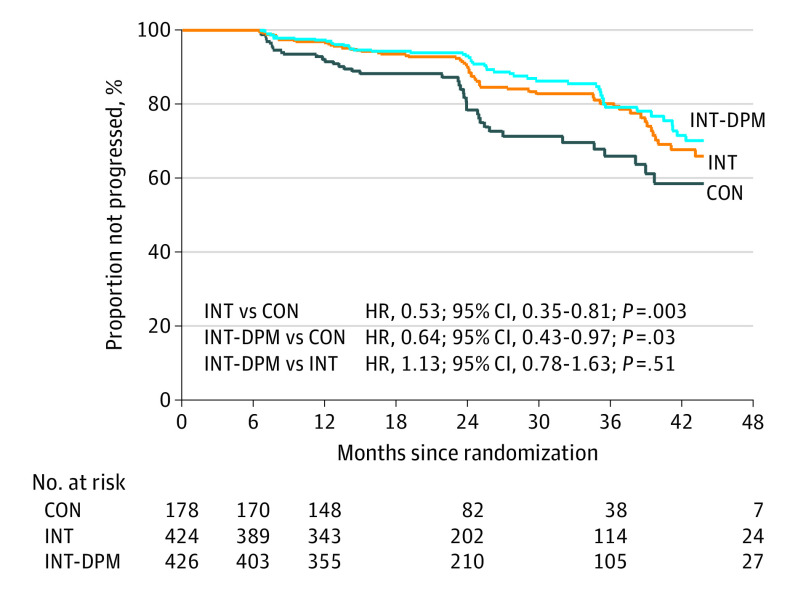
Results: In this study, 1028 participants were randomized (INT, 424 [41.2%] [166 women (39.2%)]; INT-DPM, 426 [41.4%] [147 women (34.5%)]; CON, 178 [17.3%] [70 women (%39.3)]) between January 1, 2011, and February 24, 2017. The mean (SD) age was 65.3 (10.0) years, mean (SD) body mass index 31.2 (5) (calculated as weight in kilograms divided by height in meters squared), and mean (SD) follow-up 24.7 (13.4) months. A total of 156 participants progressed to type 2 diabetes, which comprised 39 of 171 receiving CON (22.8%), 55 of 403 receiving INT (13.7%), and 62 of 414 receiving INT-DPM (15.0%). There was no significant difference between the intervention arms in the primary outcome (odds ratio [OR], 1.14; 95% CI, 0.77-1.7; P = .51), but each intervention arm had significantly lower odds of type 2 diabetes (INT: OR, 0.54; 95% CI, 0.34-0.85; P = .01; INT-DPM: OR, 0.61; 95% CI, 0.39-0.96; P = .033; combined: OR, 0.57; 95% CI, 0.38-0.87; P = .01). The effect size was similar in all glycemic, age, and social deprivation groups, and intervention costs per participant were low at $153 (£122).
Conclusions and relevance: The Norfolk Diabetes Prevention lifestyle intervention reduced the risk of type 2 diabetes in current high-risk glycemic categories. Enhancing the intervention with DPM did not further reduce diabetes risk. These translatable results are relevant for current diabetes prevention efforts.
Trial registration: ISRCTN Registry Identifier: ISRCTN34805606.
Conflict of interest statement
Figures

Comment in
-
Preventing a diabetes pandemic through lifestyle intervention.Eur Heart J. 2021 Jan 20;42(3):226-227. doi: 10.1093/eurheartj/ehaa1018. Eur Heart J. 2021. PMID: 33400772 No abstract available.
Similar articles
-
Effects of the Norfolk diabetes prevention lifestyle intervention (NDPS) on glycaemic control in screen-detected type 2 diabetes: a randomised controlled trial.BMC Med. 2021 Aug 19;19(1):183. doi: 10.1186/s12916-021-02053-x. BMC Med. 2021. PMID: 34407811 Free PMC article. Clinical Trial.
-
Study Protocol: The Norfolk Diabetes Prevention Study [NDPS]: a 46 month multi - centre, randomised, controlled parallel group trial of a lifestyle intervention [with or without additional support from lay lifestyle mentors with Type 2 diabetes] to prevent transition to Type 2 diabetes in high risk groups with non - diabetic hyperglycaemia, or impaired fasting glucose.BMC Public Health. 2017 Jan 6;17(1):31. doi: 10.1186/s12889-016-3929-5. BMC Public Health. 2017. PMID: 28056894 Free PMC article. Clinical Trial.
-
Effects of a Lifestyle Intervention to Prevent Deterioration in Glycemic Status Among South Asian Women With Recent Gestational Diabetes: A Randomized Clinical Trial.JAMA Netw Open. 2022 Mar 1;5(3):e220773. doi: 10.1001/jamanetworkopen.2022.0773. JAMA Netw Open. 2022. PMID: 35234881 Free PMC article. Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Alpha-glucosidase inhibitors for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk of developing type 2 diabetes mellitus.Cochrane Database Syst Rev. 2018 Dec 28;12(12):CD005061. doi: 10.1002/14651858.CD005061.pub3. Cochrane Database Syst Rev. 2018. PMID: 30592787 Free PMC article.
Cited by
-
Construction and Validation of a Model for Predicting Impaired Fasting Glucose Based on More Than 4000 General Population.Int J Gen Med. 2023 Apr 19;16:1415-1428. doi: 10.2147/IJGM.S409426. eCollection 2023. Int J Gen Med. 2023. PMID: 37155467 Free PMC article.
-
Evaluating the Short-Term Costs and Benefits of a Nationwide Diabetes Prevention Programme in England: Retrospective Observational Study.Appl Health Econ Health Policy. 2023 Nov;21(6):891-903. doi: 10.1007/s40258-023-00830-8. Epub 2023 Oct 3. Appl Health Econ Health Policy. 2023. PMID: 37787972 Free PMC article.
-
Incidence of diabetes mellitus following hospitalisation for COVID-19 in the United Kingdom: A prospective observational study.Diabetes Obes Metab. 2025 Feb;27(2):767-776. doi: 10.1111/dom.16071. Epub 2024 Nov 20. Diabetes Obes Metab. 2025. PMID: 39563623 Free PMC article.
-
Polygenic Risk Score, Lifestyles, and Type 2 Diabetes Risk: A Prospective Chinese Cohort Study.Nutrients. 2023 Apr 29;15(9):2144. doi: 10.3390/nu15092144. Nutrients. 2023. PMID: 37432247 Free PMC article.
-
Insights from search summary tables for evidence and gap maps: a case study on peer support interventions.J Med Libr Assoc. 2025 Apr 18;113(2):177-183. doi: 10.5195/jmla.2025.1831. J Med Libr Assoc. 2025. PMID: 40342303 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
