

Characterization of the Tumor Immune Microenvironment Identifies M0 Macrophage-Enriched Cluster as a Poor Prognostic Factor in Hepatocellular Carcinoma
- PMID: 33136432
- PMCID: PMC7713549
- DOI: 10.1200/CCI.20.00077
Characterization of the Tumor Immune Microenvironment Identifies M0 Macrophage-Enriched Cluster as a Poor Prognostic Factor in Hepatocellular Carcinoma
Abstract
Purpose: Hepatocellular carcinoma (HCC) is characterized by a poor prognosis and a high recurrence rate. The tumor immune microenvironment in HCC has been characterized as shifted toward immunosuppression. We conducted a genomic data-driven classification of immune microenvironment HCC subtypes. In addition, we demonstrated their prognostic value and suggested a potential therapeutic targeting strategy.
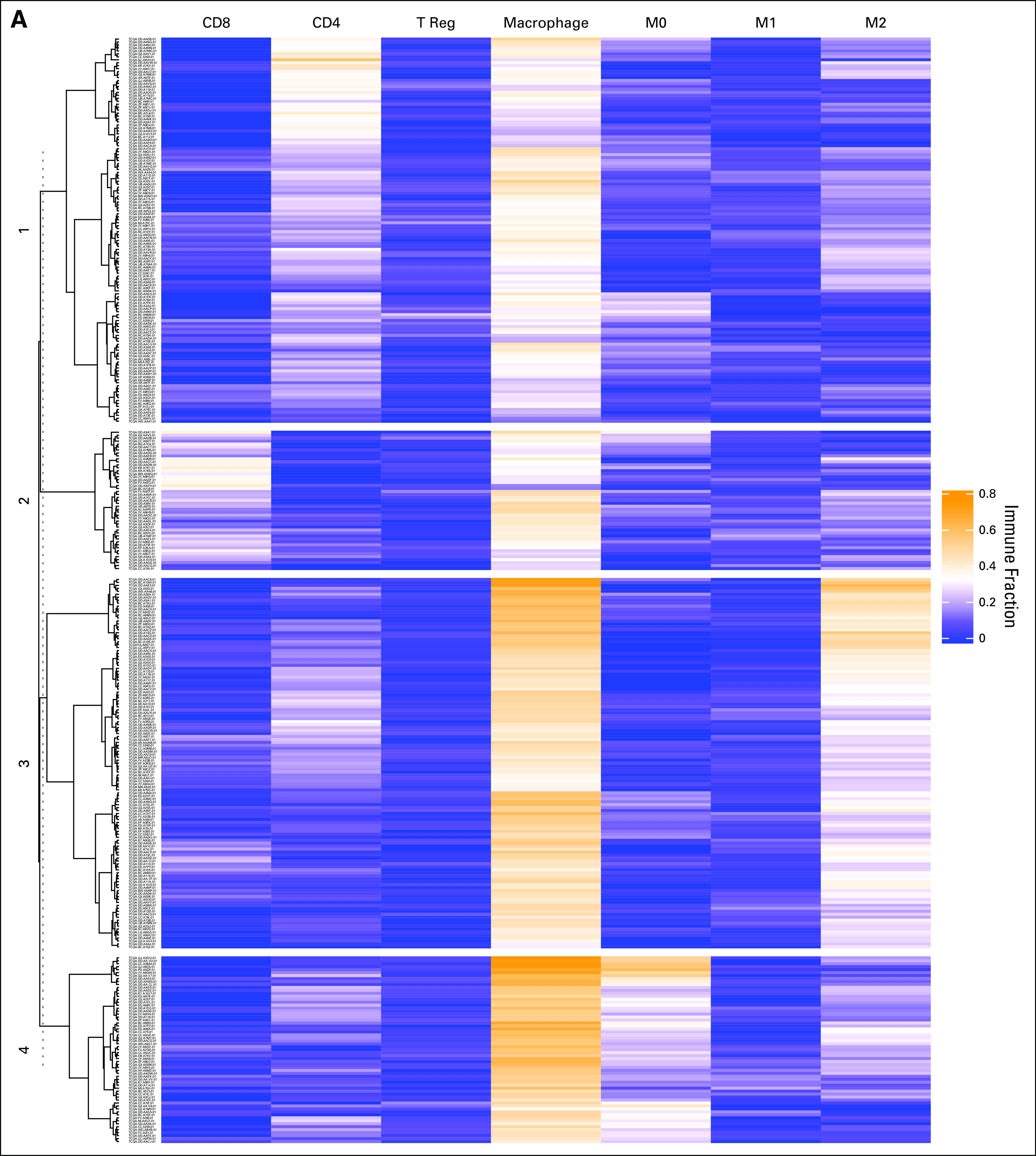
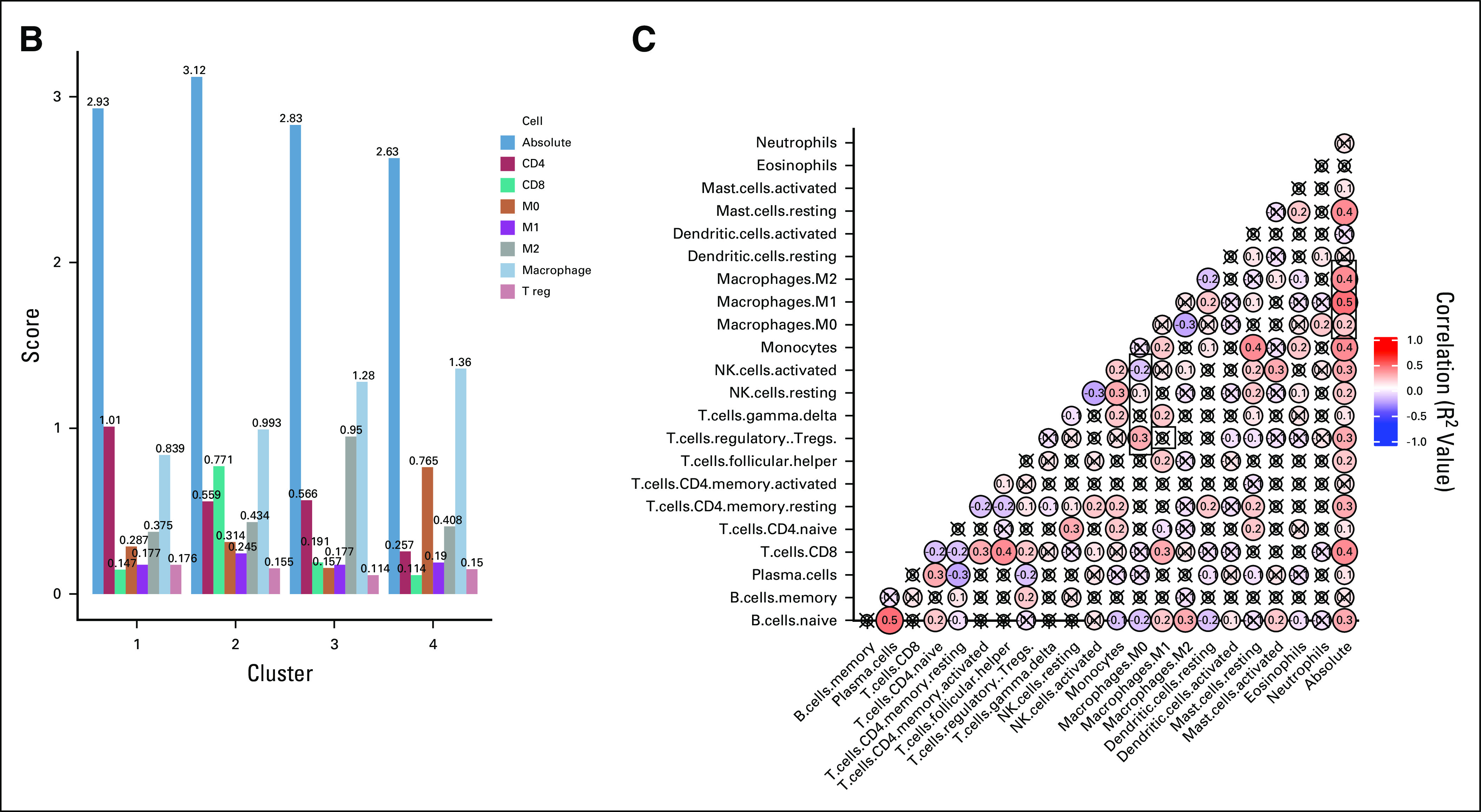
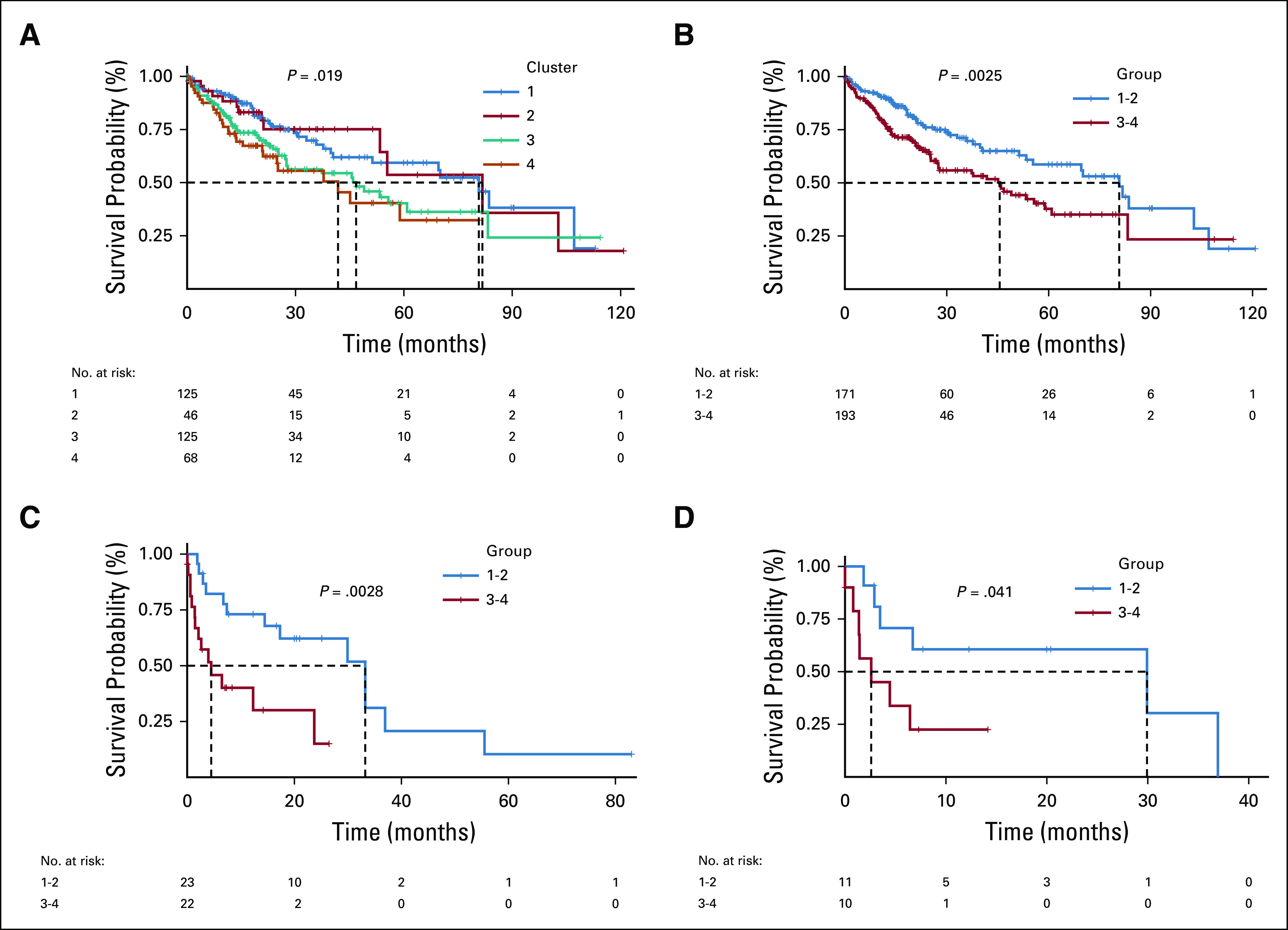
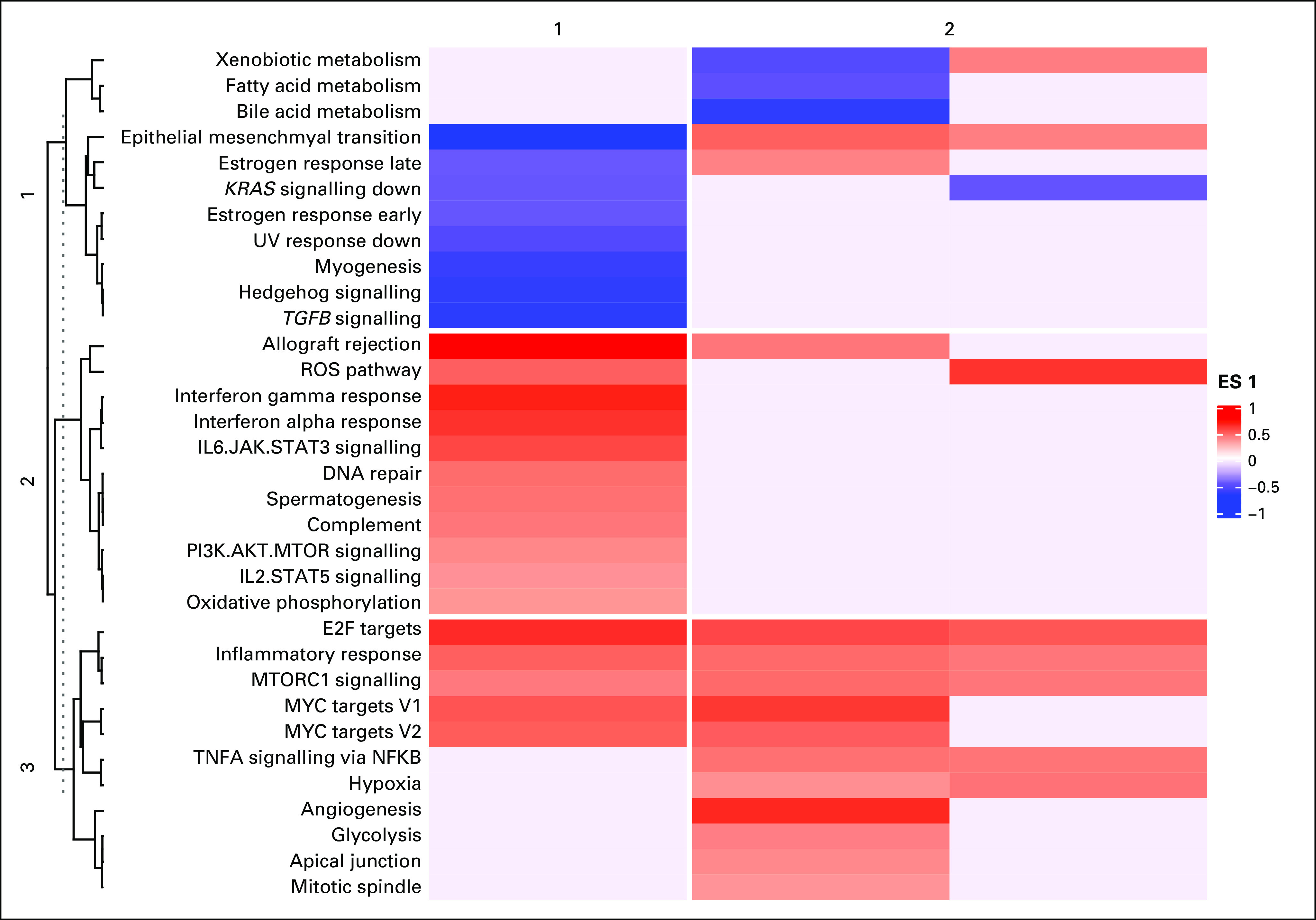
Methods: RNA sequencing data from The Cancer Genome Atlas-Liver Hepatocellular Carcinoma was used (n = 366). Abundance of immune cells was imputed using CIBERSORT and visualized using unsupervised hierarchic clustering. Overall survival (OS) was analyzed using Kaplan-Meier estimates and Cox regression. Differential expression and gene set enrichment analyses were conducted on immune clusters with poor OS and high programmed death-1 (PD-1)/programmed death-ligand 1 (PD-L1) coexpression. A scoring metric combining differentially expressed genes and immune cell content was created, and its prognostic value and immune checkpoint blockade response prediction was evaluated.
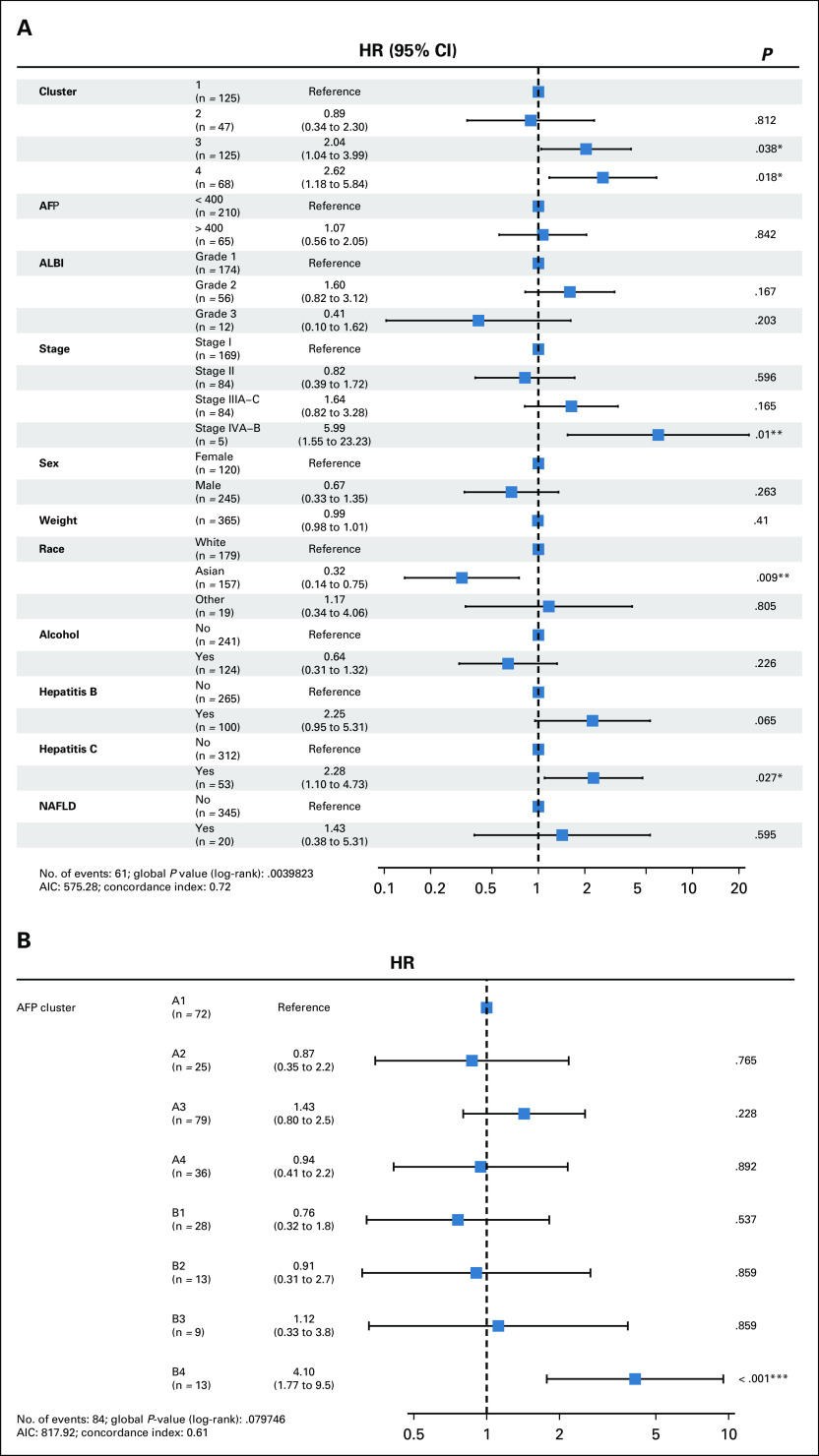
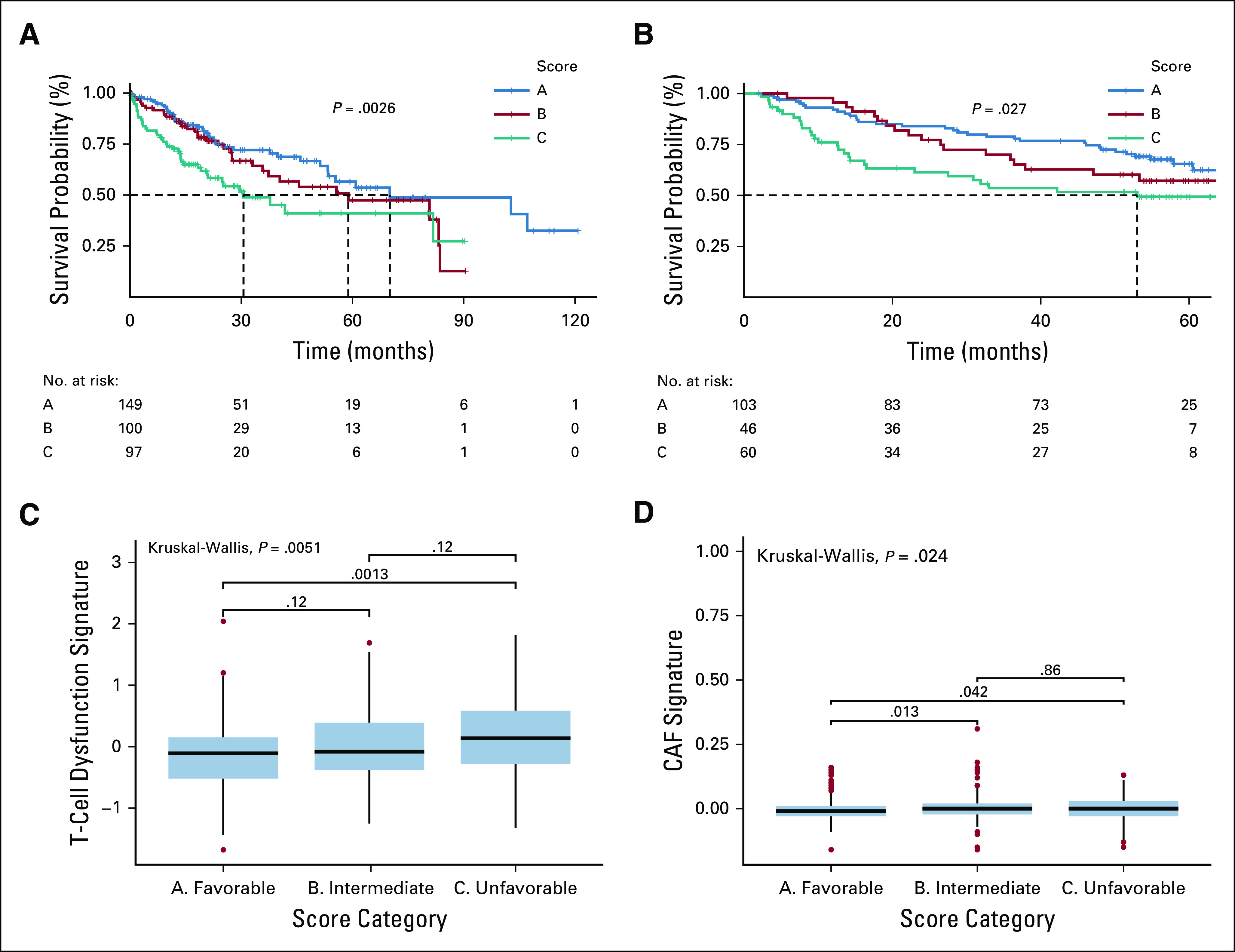
Results: Two clusters were characterized by macrophage enrichment, with distinct M0Hi and M2Hi subtypes. M2Hi (P = .038) and M0Hi (P = .018) were independently prognostic for OS on multivariable analysis. Kaplan-Meier estimates demonstrated that patients in M0Hi and M2Hi treated with sorafenib had decreased OS (P = .041), and angiogenesis hallmark genes were enriched in the M0Hi group. CXCL6 and POSTN were overexpressed in both the M0Hi and the PD-1Hi/PD-L1Hi groups. A score consisting of CXCL6 and POSTN expression and absolute M0 macrophage content was discriminatory for OS (intermediate: hazard ratio [HR], 1.59; P ≤ .001; unfavorable: HR, 2.08; P = .04).
Conclusion: Distinct immune cell clusters with macrophage predominance characterize an aggressive HCC phenotype, defined molecularly by angiogenic gene enrichment and clinically by poor prognosis and sorafenib response. This novel immunogenomic signature may aid in stratification of unresectable patients to receive checkpoint inhibitor and antiangiogenic therapy combinations.
Conflict of interest statement
Issam El Naqa
No other potential conflicts of interest were reported.
Figures
Similar articles
-
Tumor Immune Microenvironment Clusters in Localized Prostate Adenocarcinoma: Prognostic Impact of Macrophage Enriched/Plasma Cell Non-Enriched Subtypes.J Clin Med. 2020 Jun 24;9(6):1973. doi: 10.3390/jcm9061973. J Clin Med. 2020. PMID: 32599760 Free PMC article.
-
Construction and validation of an angiogenesis-related scoring model to predict prognosis, tumor immune microenvironment and therapeutic response in hepatocellular carcinoma.Front Immunol. 2022 Nov 17;13:1013248. doi: 10.3389/fimmu.2022.1013248. eCollection 2022. Front Immunol. 2022. PMID: 36466855 Free PMC article.
-
Prognostic value of intratumoral lymphocyte-to-monocyte ratio and M0 macrophage enrichment in tumor immune microenvironment of melanoma.Melanoma Manag. 2020 Nov 2;7(4):MMT51. doi: 10.2217/mmt-2020-0019. Melanoma Manag. 2020. PMID: 33318782 Free PMC article.
-
Screening and identification of angiogenesis-related genes as potential novel prognostic biomarkers of hepatocellular carcinoma through bioinformatics analysis.Aging (Albany NY). 2021 Jul 12;13(13):17707-17733. doi: 10.18632/aging.203260. Epub 2021 Jul 12. Aging (Albany NY). 2021. PMID: 34252885 Free PMC article.
-
Viral status, immune microenvironment and immunological response to checkpoint inhibitors in hepatocellular carcinoma.J Immunother Cancer. 2020 Apr;8(1):e000394. doi: 10.1136/jitc-2019-000394. J Immunother Cancer. 2020. PMID: 32303615 Free PMC article.
Cited by
-
Machine learning-based identification of telomere-related gene signatures for prognosis and immunotherapy response in hepatocellular carcinoma.Mol Cytogenet. 2025 Mar 18;18(1):6. doi: 10.1186/s13039-025-00705-8. Mol Cytogenet. 2025. PMID: 40102883 Free PMC article.
-
Transcriptomic analysis of Paraoxonase 1 expression in hepatocellular carcinoma and its potential impact on tumor immunity.Clin Transl Oncol. 2025 Feb;27(2):612-629. doi: 10.1007/s12094-024-03598-y. Epub 2024 Jul 20. Clin Transl Oncol. 2025. PMID: 39031295
-
EPHX2 Inhibits Colon Cancer Progression by Promoting Fatty Acid Degradation.Front Oncol. 2022 Mar 30;12:870721. doi: 10.3389/fonc.2022.870721. eCollection 2022. Front Oncol. 2022. PMID: 35433439 Free PMC article.
-
Identification of Hub Genes and Immune Infiltration in Non-alcoholic Fatty Liver Disease -Related Hepatocellular Carcinoma by Bioinformatics Analysis.Turk J Gastroenterol. 2023 Apr;34(4):383-393. doi: 10.5152/tjg.2023.22590. Turk J Gastroenterol. 2023. PMID: 37089050 Free PMC article.
-
Bioinformation study of immune microenvironment characteristics of disulfidptosis-related subtypes in ovarian cancer and prognostic model construction.Discov Oncol. 2025 Jan 8;16(1):18. doi: 10.1007/s12672-025-01752-8. Discov Oncol. 2025. PMID: 39775403 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
-
- Center MM, Jemal A. International trends in liver cancer incidence rates. Cancer Epidemiol Biomarkers Prev. 2011;20:2362–2368. - PubMed
-
- Perz JF, Armstrong GL, Farrington LA, et al. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529–538. - PubMed
-
- Sanyal AJ, Yoon SK, Lencioni R. The etiology of hepatocellular carcinoma and consequences for treatment. Oncologist. 2010;15(suppl 4):14–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
