

Operationalization of the Brief ICF Core Set for Hearing Loss: An ICF-Based e-Intake Tool in Clinical Otology and Audiology Practice
- PMID: 33136629
- PMCID: PMC7722460
- DOI: 10.1097/AUD.0000000000000867
Operationalization of the Brief ICF Core Set for Hearing Loss: An ICF-Based e-Intake Tool in Clinical Otology and Audiology Practice
Abstract
Objectives: According to the International Classification of Functioning, Disability and Health (ICF), functioning reflects the interplay between an individual's body structures and functions, activities, participation, environmental, and personal factors. To be useful in clinical practice, these concepts need to be operationalized into a practical and integral instrument. The Brief ICF Core Set for Hearing Loss (CSHL) provides a minimum standard for the assessment of functioning in adults with hearing loss. The objective of the present study was to operationalize the Brief CSHL into a digital intake tool that could be used in the otology-audiology practice for adults with ear and hearing problems as part of their intake assessment.
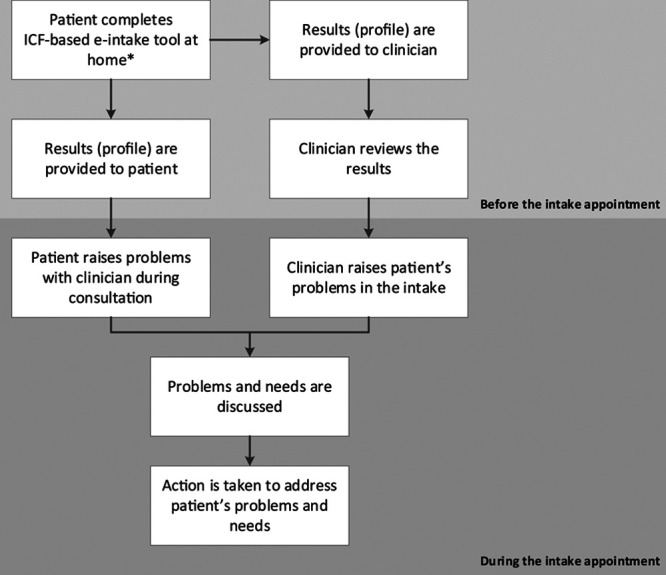
Design: A three-step approach was followed: (1) Selecting and formulating questionnaire items and response formats, using the 27 categories of the Brief CSHL as a basis. Additional categories were selected based on relevant literature and clinical expertise. Items were selected from existing, commonly used disease-specific questionnaires, generic questionnaires, or the WHO's official descriptions of ICF categories. The response format was based on the existing item's response categories or on the ICF qualifiers. (2) Carrying out an expert survey and a pilot study (using the three-step test interview. Relevant stakeholders and patients were asked to comment on the relevance, comprehensiveness, and comprehensibility of the items. Results were discussed in the project group, and items were modified based on consensus. (3) Integration of the intake tool into a computer-based system for use in clinical routine.
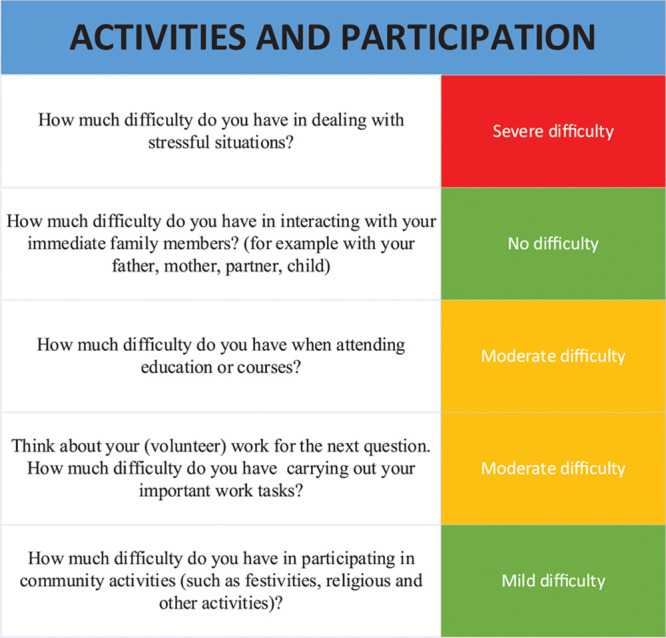
Results: The Brief CSHL was operationalized into 62 items, clustered into six domains: (1) general information, including reason for visit, sociodemographic, and medical background; (2) general body functions; (3) ear and hearing structures and functions; (4) activities and participation (A&P); (5) environmental factors (EF); and (6) personal factors (mastery and coping). Based on stakeholders' responses, the instructions of the items on A&P and EF were adapted. The three-step test interview showed that the tool had sufficient content validity but that some items on EF were redundant. Overall, the stakeholders and patients indicated that the intake tool was relevant and had a logical and clear structure. The tool was integrated in an online portal.
Conclusions: In the current study, an ICF-based e-intake tool was developed that aims to screen self-reported functioning problems in adults with an ear/hearing problem. The relevance, comprehensiveness, and comprehensibility of the originally proposed item list was supported, although the stakeholder and patient feedback resulted into some changes of the tool on item-level. Ultimately, the functioning information obtained with the tool could be used to promote patient-centered ear and hearing care taking a biopsychosocial perspective into account.
Conflict of interest statement
The authors report no conflict of interest. The authors alone are responsible for the content and writing of this article.
Figures
References
-
- Alfakir R., Hall M., Holmes A. E. How can the success post cochlear implant be measured or defined in older adults? Implications of the International Classification of Functioning Brief Core Set for Hearing Loss. Int J Phys Med Rehabil, (2015a). 32
-
- Alfakir R., Holmes A. E., Noreen F. Functional performance in older adults with hearing loss: Application of the International Classification of Functioning Brief Core Set for Hearing Loss: A pilot study. Int J Audiol, (2015b). 54:579–586. - PubMed
-
- Alfakir R., van Leeuwen L. M., Pronk M., et al. Comparing the International Classification of Functioning, Disability, and Health Core Sets for Hearing Loss and Otorhinolaryngology/Audiology Intake Documentation at Mayo Clinic. Ear Hear, (2019). 40:858–869. - PubMed
-
- Asplund R. Sleepiness and sleep in elderly subjects with hearing complaints. Arch Gerontol Geriatr, (2003). 36:93–99. - PubMed
-
- Barker A. B., Leighton P., Ferguson M. A. Coping together with hearing loss: A qualitative meta-synthesis of the psychosocial experiences of people with hearing loss and their communication partners. Int J Audiol, (2017). 56:297–305. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
