

Long-Acting Injectable Cabotegravir + Rilpivirine for HIV Maintenance Therapy: Week 48 Pooled Analysis of Phase 3 ATLAS and FLAIR Trials
- PMID: 33136751
- PMCID: PMC7592884
- DOI: 10.1097/QAI.0000000000002466
Long-Acting Injectable Cabotegravir + Rilpivirine for HIV Maintenance Therapy: Week 48 Pooled Analysis of Phase 3 ATLAS and FLAIR Trials
Abstract
Background: Long-acting (LA) injectable regimens are a potential therapeutic option in people living with HIV-1.
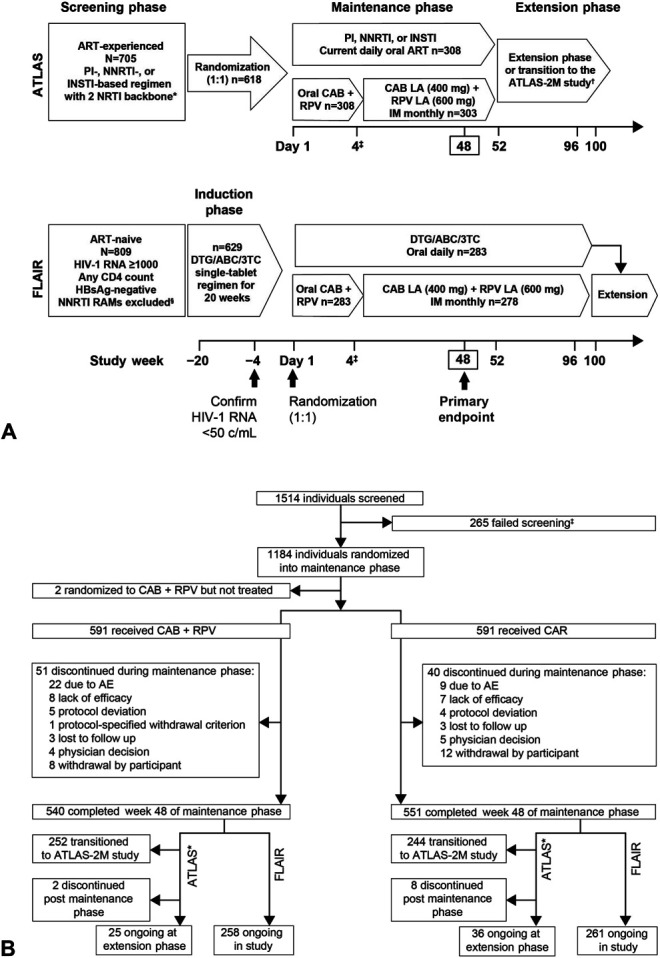
Setting: ATLAS (NCT02951052) and FLAIR (NCT02938520) were 2 randomized, open-label, multicenter, multinational phase 3 studies.
Methods: Adult participants with virologic suppression (plasma HIV-1 RNA <50 copies/mL) were randomized (1:1) to continue with their current antiretroviral regimen (CAR) or switch to the long-acting (LA) regimen of cabotegravir (CAB) and rilpivirine (RPV). In the LA arm, participants initially received oral CAB + RPV once-daily for 4 weeks to assess individual safety and tolerability, before starting monthly injectable therapy. The primary endpoint of this combined analysis was antiviral efficacy at week 48 (FDA Snapshot algorithm: noninferiority margin of 4% for HIV-1 RNA ≥50 copies/mL). Safety, tolerability, and confirmed virologic failure (2 consecutive plasma HIV-1 RNA ≥200 copies/mL) were secondary endpoints.
Results: The pooled intention-to-treat exposed population included 591 participants in each arm [28% women (sex at birth), 19% aged ≥50 years]. Noninferiority criteria at week 48 were met for the primary (HIV-1 RNA ≥50 copies/mL) and key secondary (HIV-1 RNA <50 copies/mL) efficacy endpoints. Seven individuals in each arm (1.2%) developed confirmed virologic failure; 6/7 (LA) and 3/7 (CAR) had resistance-associated mutations. Most LA recipients (83%) experienced injection site reactions, which decreased in incidence over time. Injection site reactions led to the withdrawal of 6 (1%) participants. The serious adverse event rate was 4% in each arm.
Conclusion: This combined analysis demonstrates monthly injections of CAB + RPV LA were noninferior to daily oral CAR for maintaining HIV-1 suppression.
Conflict of interest statement
G.R. has received grants and personal fees from MSD, Gilead, and ViiV Healthcare; grants from Janssen, outside of the submitted work. E.T.O. has received research support to institution during the conduct of this study, and has served as a consultant for ViiV, Merck, Theratechnologies, and Gilead outside of the submitted work. C.O. reports grants, personal fees, and non-financial support from ViiV Healthcare during the conduct of the study, and grants, personal fees, non-financial support, and other from Gilead, MSD, Janssen, ViiV, and GlaxoSmithKline outside of the submitted work. S.S. reports grants to her institution from ViiV Healthcare during the conduct of this study. K.A. reports grants from ViiV Healthcare and GlaxoSmithKline outside of the submitted work. M.G.H.-M. reports personal fees from ViiV Healthcare, during the conduct of the study; grants and personal fees from ViiV Healthcare, personal fees from Gilead, personal fees from Janssen, outside the submitted work. V.P. has received personal fees from GlaxoSmithKline, Gilead, MSD, and ViiV Healthcare and non-financial support from GlaxoSmithKline outside of the submitted work. S.O. reports grants from MSD and ViiV Healthcare; honorarium for lectures from MSD, ViiV Healthcare, Gilead, Torii Pharmaceutical, and Janssen; non-financial support from Japan Tobacco/Torii Pharmaceutical, outside of the submitted work. G.J.R. has received grants from Gilead, ViiV Healthcare, TaiMed outside of the submitted work. A.B. has received personal fees (honoraria) from AbbVie, Gilead, Janssen, Sanofi, MSD, and ViiV Healthcare outside of the submitted work. M.M. has received consulting fees for advisory boards from ViiV Healthcare, Janssen and Gilead, and travel grants from ViiV Healthcare and Janssen, outside of the submitted work. S.G., C.H., K.H., M.S.C., C.T., P.P., A.C., R.D., J.M., K.S., W.S., and D.M. are employed by ViiV Healthcare. V.V.E., S.V., R.V.S.-R., and H.C. are employed by Janssen. S.F., S.W., K.C., J.R., A.W., and N.W. are employed by GlaxoSmithKline. K.S., D.M., J.M., W.S., C.T., S.F., A.C., S.G., K.H., P.P., and R.D. are stockholders of GlaxoSmithKline. M.S.C. reports company stock options at GlaxoSmithKline. C.H. is a shareholder of GlaxoSmithKline. S.V. and H.C. are shareholders of Johnson & Johnson. The remaining authors have no conflicts of interest to disclose.
Figures
References
-
- UNAIDS. Global HIV & AIDS Statistics—2019 Fact Sheet. 2019. Available at: https://www.unaids.org/en/resources/fact-sheet. Accessed October 31, 2019.
-
- World Health Organization. Summary of the Global HIV Epidemic. 2018. Available at: https://www.who.int/gho/hiv/en/. Accessed October 31, 2019.
-
- Nachega JB, Hsu AJ, Uthman OA, et al. Antiretroviral therapy adherence and drug-drug interactions in the aging HIV population. AIDS. 2012;26(suppl 1):S39–S53. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
