

Incidence and outcome of out-of-hospital cardiac arrests in the COVID-19 era: A systematic review and meta-analysis
- PMID: 33137418
- PMCID: PMC7603976
- DOI: 10.1016/j.resuscitation.2020.10.025
Incidence and outcome of out-of-hospital cardiac arrests in the COVID-19 era: A systematic review and meta-analysis
Abstract
Background: The impact of COVID-19 on pre-hospital and hospital services and hence on the prevalence and outcomes of out-of-hospital cardiac arrests (OHCA) remain unclear. The review aimed to evaluate the influence of the COVID-19 pandemic on the incidence, process, and outcomes of OHCA.
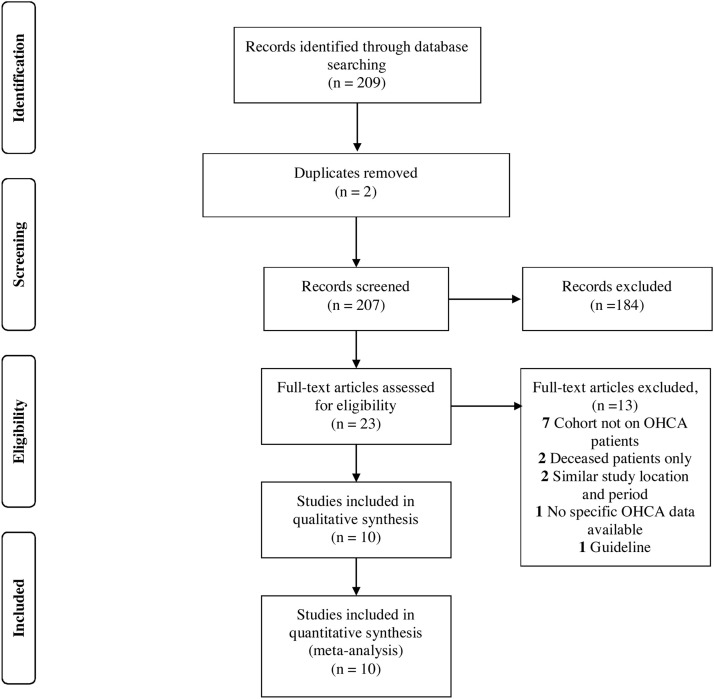
Methods: A systematic review of PubMed, EMBASE, and pre-print websites was performed. Studies reporting comparative data on OHCA within the same jurisdiction, before and during the COVID-19 pandemic were included. Study quality was assessed based on the Newcastle-Ottawa Scale.
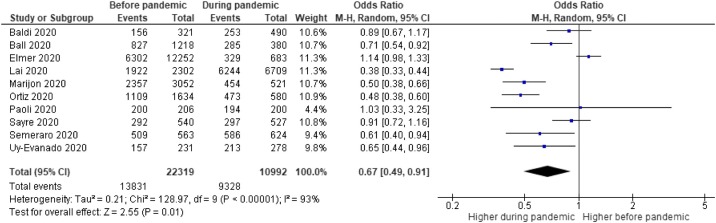
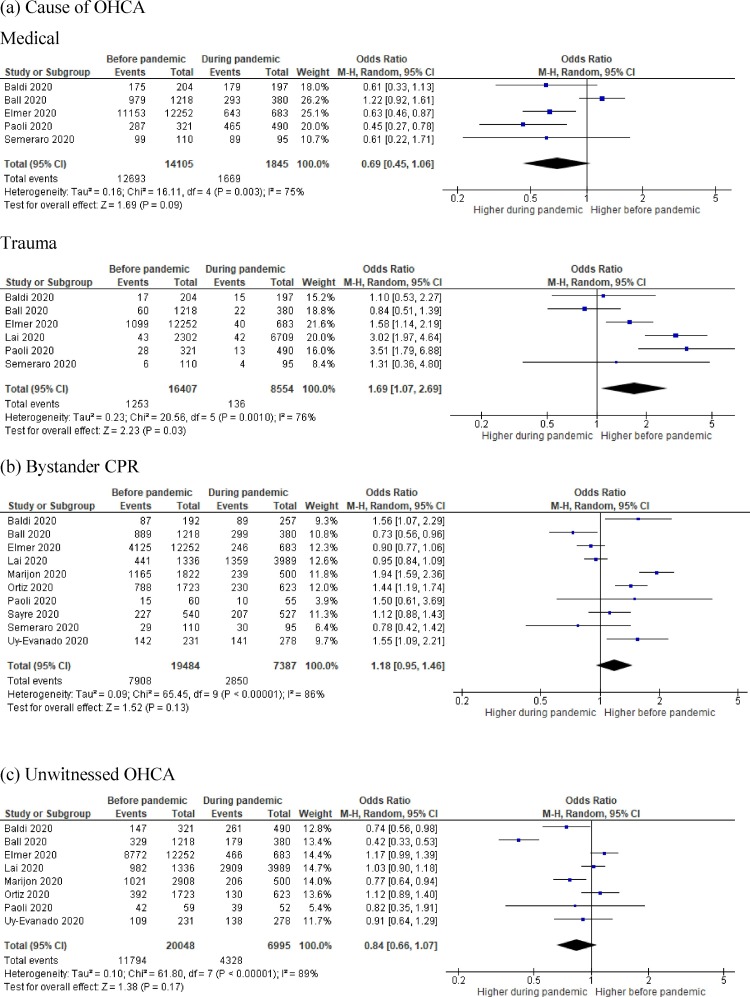
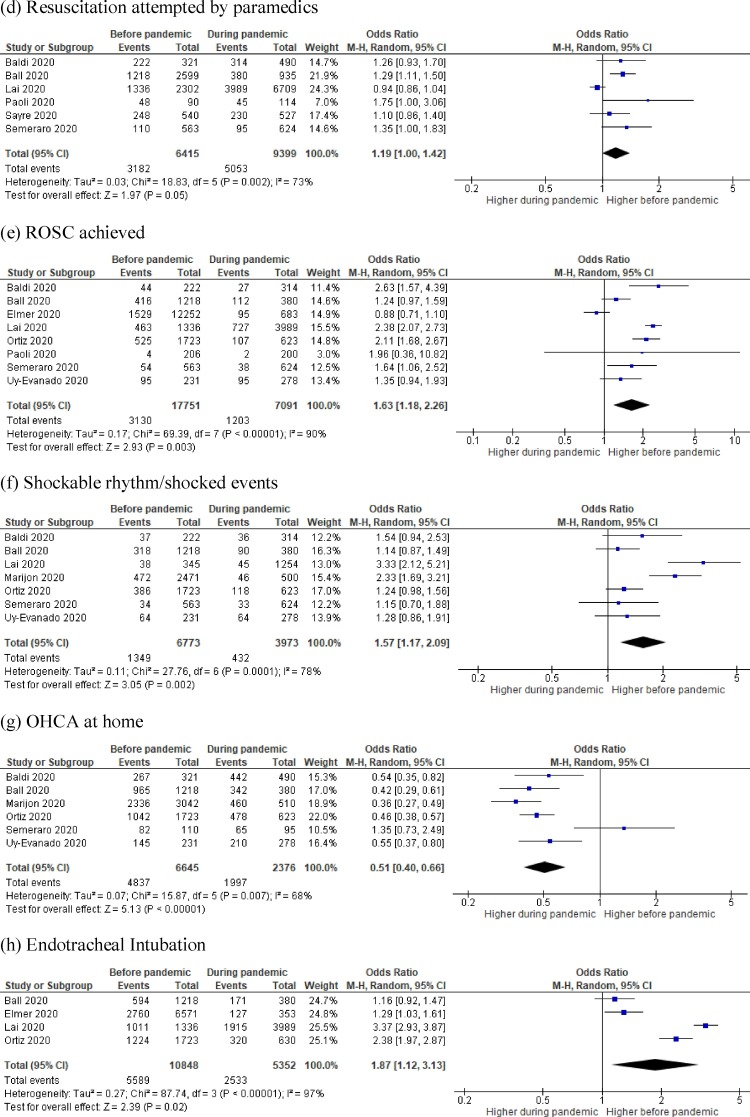
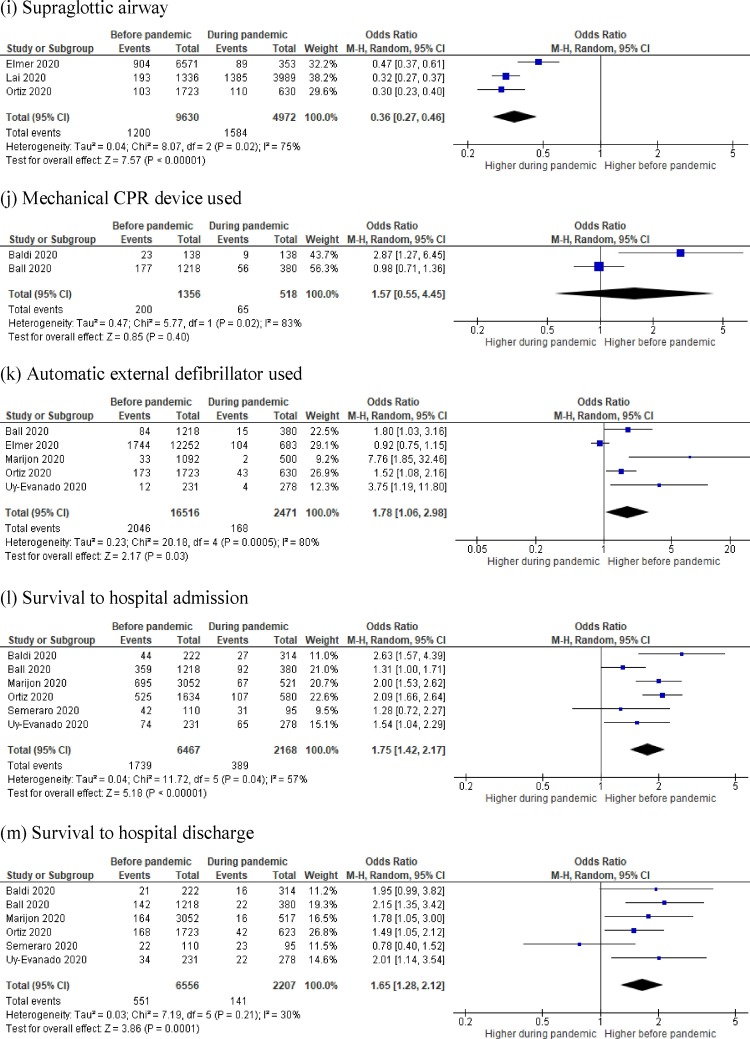
Results: Ten studies reporting data from 35,379 OHCA events were included. There was a 120% increase in OHCA events since the pandemic. Time from OHCA to ambulance arrival was longer during the pandemic (p = 0.036). While mortality (OR = 0.67, 95%-CI 0.49-0.91) and supraglottic airway use (OR = 0.36, 95%-CI 0.27-0.46) was higher during the pandemic, automated external defibrillator use (OR = 1.78 95%-CI 1.06-2.98), return of spontaneous circulation (OR = 1.63, 95%CI 1.18-2.26) and intubation (OR = 1.87, 95%-CI 1.12--3.13) was more common before the pandemic. More patients survived to hospital admission (OR = 1.75, 95%-CI 1.42-2.17) and discharge (OR = 1.65, 95%-CI 1.28-2.12) before the pandemic. Bystander CPR (OR = 1.18, 95%-CI 0.95-1.46), unwitnessed OHCA (OR = 0.84, 95%-CI 0.66-1.07), paramedic-resuscitation attempts (OR = 1.19 95%-CI 1.00-1.42) and mechanical CPR device use (OR = 1.57 95%-CI 0.55-4.55) did not defer significantly.
Conclusions: The incidence and mortality following OHCA was higher during the COVID-19 pandemic. There were significant variations in resuscitation practices during the pandemic. Research to define optimal processes of pre-hospital care during a pandemic is urgently required.
Review registration: PROSPERO (CRD42020203371).
Keywords: COVID-19; Cardiac arrest; OHCA; Out of hospital; SARS-CoV-2.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors report no declarations of interest.
Figures
Comment in
-
COVID-19 and the global OHCA crisis: An urgent need for system level solutions.Resuscitation. 2020 Dec;157:274-276. doi: 10.1016/j.resuscitation.2020.11.004. Epub 2020 Nov 9. Resuscitation. 2020. PMID: 33181230 Free PMC article. No abstract available.
References
-
- World Health Organisation . 2020. Coronavirus disease (COVID-19) Situation reports.
-
- Bossaert L.L. Fibrillation and defibrillation of the heart. Br J Anaesth. 1997;79:203–213. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
