

Aging in COVID-19: Vulnerability, immunity and intervention
- PMID: 33137510
- PMCID: PMC7604159
- DOI: 10.1016/j.arr.2020.101205
Aging in COVID-19: Vulnerability, immunity and intervention
Abstract
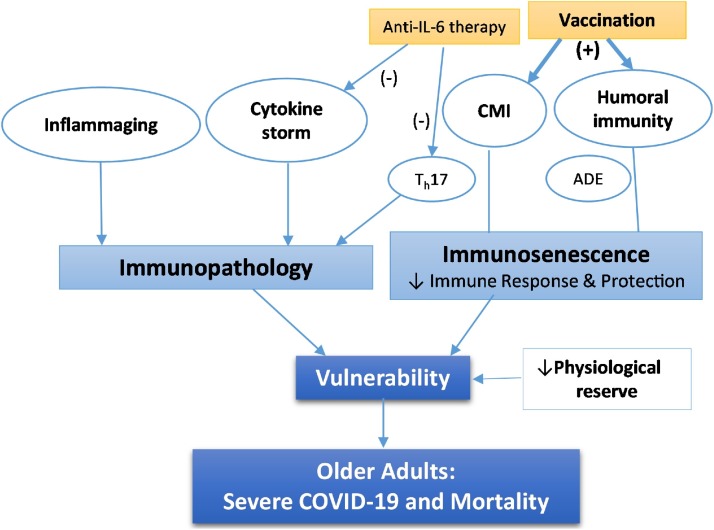
The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) pandemic was first reported in Wuhan, China in December 2019, moved across the globe at an unprecedented speed, and is having a profound and yet still unfolding health and socioeconomic impacts. SARS-CoV-2, a β-coronavirus, is a highly contagious respiratory pathogen that causes a disease that has been termed the 2019 coronavirus disease (COVID-19). Clinical experience thus far indicates that COVID-19 is highly heterogeneous, ranging from being asymptomatic and mild to severe and causing death. Host factors including age, sex, and comorbid conditions are key determinants of disease severity and progression. Aging itself is a prominent risk factor for severe disease and death from COVID-19. We hypothesize that age-related decline and dysregulation of immune function, i.e., immunosenescence and inflammaging play a major role in contributing to heightened vulnerability to severe COVID-19 outcomes in older adults. Much remains to be learned about the immune responses to SARS-CoV-2 infection. We need to begin partitioning all immunological outcome data by age to better understand disease heterogeneity and aging. Such knowledge is critical not only for understanding of COVID-19 pathogenesis but also for COVID-19 vaccine development.
Keywords: Aging; Anti-IL-6 therapy; COVID-19; Cytokine storm; Immunopathology; Immunosenescence; Inflammaging; SARS-CoV-2; Vaccination.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Comment in
-
Cellular senescence is a potential severity factor for COVID-19: Suitable targets required to eliminate cellular senescence.Respir Med. 2021 Sep;186:106517. doi: 10.1016/j.rmed.2021.106517. Epub 2021 Jun 21. Respir Med. 2021. PMID: 34186259 Free PMC article. No abstract available.
References
-
- Akbar A.N., Gilroy D.W. Aging immunity may exacerbate COVID-19. Science. 2020;369:256–257. - PubMed
-
- Arons M.M., Hatfield K.M., Reddy S.C., Kimball A., James A., Jacobs J.R., Taylor J., Spicer K., Bardossy A.C., Oakley L.P., Tanwar S., Dyal J.W., Harney J., Chisty Z., Bell J.M., Methner M., Paul P., Carlson C.M., McLaughlin H.P., Thornburg N., Tong S., Tamin A., Tao Y., Uehara A., Harcourt J., Clark S., Brostrom-Smith C., Page L.C., Kay M., Lewis J., Montgomery P., Stone N.D., Clark T.A., Honein M.A., Duchin J.S., Jernigan J.A., Public H.-S., King C., Team C.C.-I. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Engl. J. Med. 2020;382:2081–2090. - PMC - PubMed
-
- Arvin A.M., Fink K., Schmid M.A., Cathcart A., Spreafico R., Havenar-Daughton C., Lanzavecchia A., Corti D., Virgin H.W. A perspective on potential antibody-dependent enhancement of SARS-CoV-2. Nature. 2020;584:353–363. - PubMed
-
- Baig A.M., Khaleeq A., Ali U., Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 2020;11:995–998. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
