

MZe786, a hydrogen sulfide-releasing aspirin prevents preeclampsia in heme oxygenase-1 haplodeficient pregnancy under high soluble flt-1 environment
- PMID: 33137710
- PMCID: PMC7610044
- DOI: 10.1016/j.redox.2020.101768
MZe786, a hydrogen sulfide-releasing aspirin prevents preeclampsia in heme oxygenase-1 haplodeficient pregnancy under high soluble flt-1 environment
Abstract
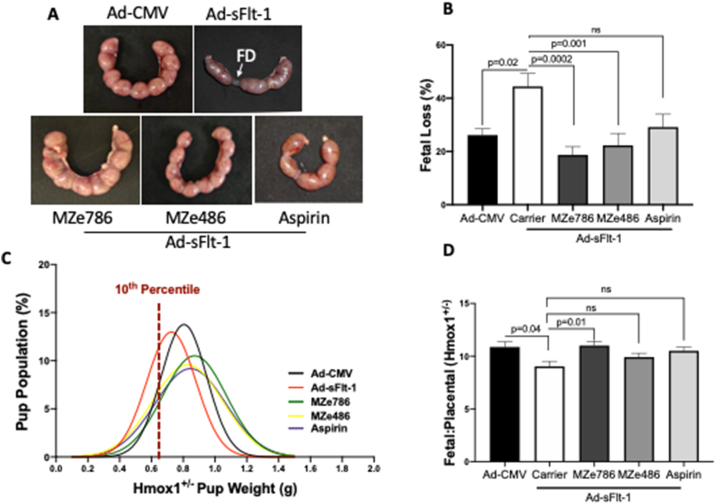
Preeclampsia affects one in twelve of the 130 million pregnancies a year. The lack of an effective therapeutic to prevent or treat it is responsible for an annual global cost burden of 100 billion US dollars. Preeclampsia also affects these women later in life as it is a recognised risk factor for cardiovascular disease, stroke and vascular dementia. Our laboratory demonstrated that preeclampsia is associated with high soluble fms-like tyrosine kinase 1 (sFlt-1) and low heme oxygenase-1 (HO1/Hmox1) expression. Here we sought to determine the therapeutic value of a novel H2S-releasing aspirin (MZe786) in HO-1 haploid deficient (Hmox1+/-) pregnant mice in a high sFlt-1 environment. Pregnant Hmox1+/- mice were injected with adenovirus encoding sFlt-1 or control virus at gestation day E11.5. Subsequently, Hmox1+/- dams were treated daily with a number of treatment regimens until E17.5, when maternal and fetal outcomes were assessed. Here we show that HO-1 compromised mice in a high sFlt-1 environment during pregnancy exhibit severe preeclampsia signs and a reduction in antioxidant genes. MZe786 ameliorates preeclampsia by reducing hypertension and renal damage possibly by stimulating antioxidant genes. MZe786 also improved fetal outcome in comparison with aspirin alone and appears to be a better therapeutic agent at preventing preeclampsia than aspirin alone.
Keywords: Heme oxygenase-1; Hydrogen sulfide; Hypertension; Preeclampsia; sFlt-1.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
HR, SA, LSA, IHKD, FAA, SwA and AS declare they have no conflict of interest. AA is the Executive Chairman and the majority shareholder in MirZyme Therapeutics. AA and KW are inventors for the use of hydrogen sulphide compounds in the treatment of preeclampsia (WO2014132083A2).
Figures




Similar articles
-
MZe786 Rescues Cardiac Mitochondrial Activity in High sFlt-1 and Low HO-1 Environment.Antioxidants (Basel). 2020 Jul 9;9(7):598. doi: 10.3390/antiox9070598. Antioxidants (Basel). 2020. PMID: 32660064 Free PMC article.
-
Hydrogen sulfide releasing molecule MZe786 inhibits soluble Flt-1 and prevents preeclampsia in a refined RUPP mouse model.Redox Biol. 2021 Jan;38:101814. doi: 10.1016/j.redox.2020.101814. Epub 2020 Nov 28. Redox Biol. 2021. PMID: 33321463 Free PMC article.
-
Molecular mechanisms and therapeutic implications of the carbon monoxide/hmox1 and the hydrogen sulfide/CSE pathways in the prevention of pre-eclampsia and fetal growth restriction.Pregnancy Hypertens. 2014 Jul;4(3):243-4. doi: 10.1016/j.preghy.2014.04.013. Epub 2014 Jul 9. Pregnancy Hypertens. 2014. PMID: 26104642
-
Therapeutic potential of statins and the induction of heme oxygenase-1 in preeclampsia.J Reprod Immunol. 2014 Mar;101-102(100):153-160. doi: 10.1016/j.jri.2013.12.120. Epub 2014 Jan 16. J Reprod Immunol. 2014. PMID: 24503248 Free PMC article. Review.
-
New insights into the etiology of preeclampsia: identification of key elusive factors for the vascular complications.Thromb Res. 2011 Feb;127 Suppl 3:S72-5. doi: 10.1016/S0049-3848(11)70020-2. Thromb Res. 2011. PMID: 21262447 Review.
Cited by
-
Region-Specific and Pregnancy-Enhanced Vasodilator Effects of Hydrogen Sulfide.Obstet Gynecol Res. 2023;6(4):309-316. doi: 10.26502/ogr0145. Epub 2023 Dec 22. Obstet Gynecol Res. 2023. PMID: 38288009 Free PMC article.
-
H2S donor GYY4137 mitigates sFlt-1-induced hypertension and vascular dysfunction in pregnant rats†.Biol Reprod. 2024 Oct 14;111(4):879-889. doi: 10.1093/biolre/ioae103. Biol Reprod. 2024. PMID: 38938086 Free PMC article.
-
Sodium Thiosulphate-Loaded Liposomes Control Hydrogen Sulphide Release and Retain Its Biological Properties in Hypoxia-like Environment.Antioxidants (Basel). 2022 Oct 24;11(11):2092. doi: 10.3390/antiox11112092. Antioxidants (Basel). 2022. PMID: 36358464 Free PMC article.
-
Advances of H2S in Regulating Neurodegenerative Diseases by Preserving Mitochondria Function.Antioxidants (Basel). 2023 Mar 6;12(3):652. doi: 10.3390/antiox12030652. Antioxidants (Basel). 2023. PMID: 36978900 Free PMC article. Review.
-
H2S Donors and Their Use in Medicinal Chemistry.Biomolecules. 2021 Dec 18;11(12):1899. doi: 10.3390/biom11121899. Biomolecules. 2021. PMID: 34944543 Free PMC article. Review.
References
-
- Wilson M.L., Goodwin T.M., Pan V.L., Ingles S.A. Molecular epidemiology of preeclampsia. Obstet. Gynecol. Surv. 2003;58(1):39–66. - PubMed
-
- Kuklina E.V., Ayala C., Callaghan W.M. Hypertensive disorders and severe obstetric morbidity in the United States. Obstet. Gynecol. 2009;113(6):1299–1306. - PubMed
-
- Schindler A.E. New data about preeclampsia: some possibilities of prevention. Gynecol. Endocrinol. 2018;34(8):636–637. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
