

Clinicopathological Features as Prognostic Predictors of Poor Outcome in Papillary Thyroid Carcinoma
- PMID: 33138175
- PMCID: PMC7693726
- DOI: 10.3390/cancers12113186
Clinicopathological Features as Prognostic Predictors of Poor Outcome in Papillary Thyroid Carcinoma
Abstract
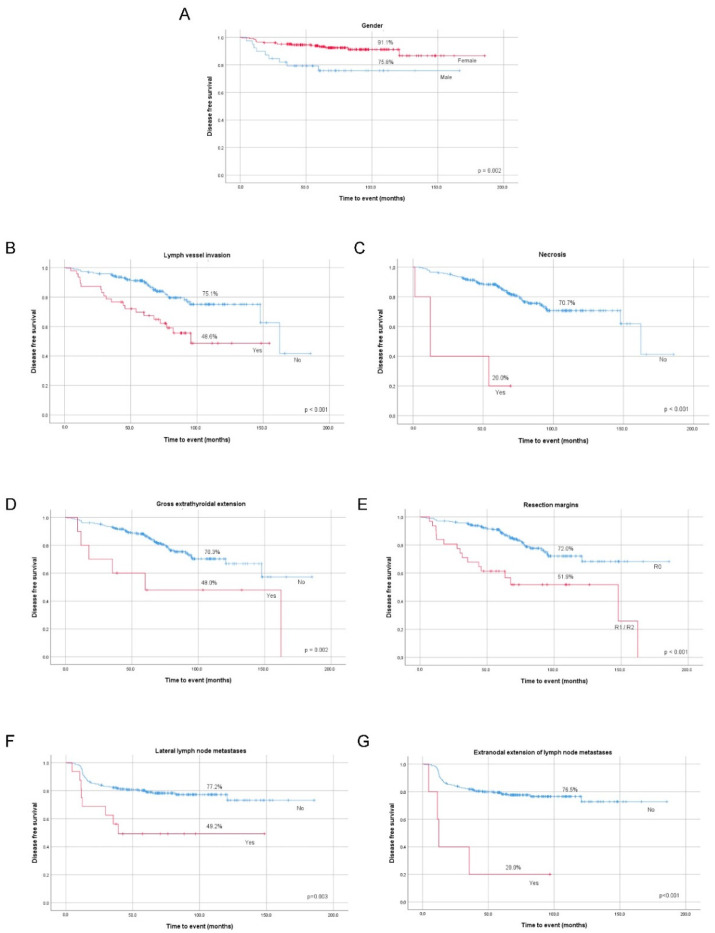
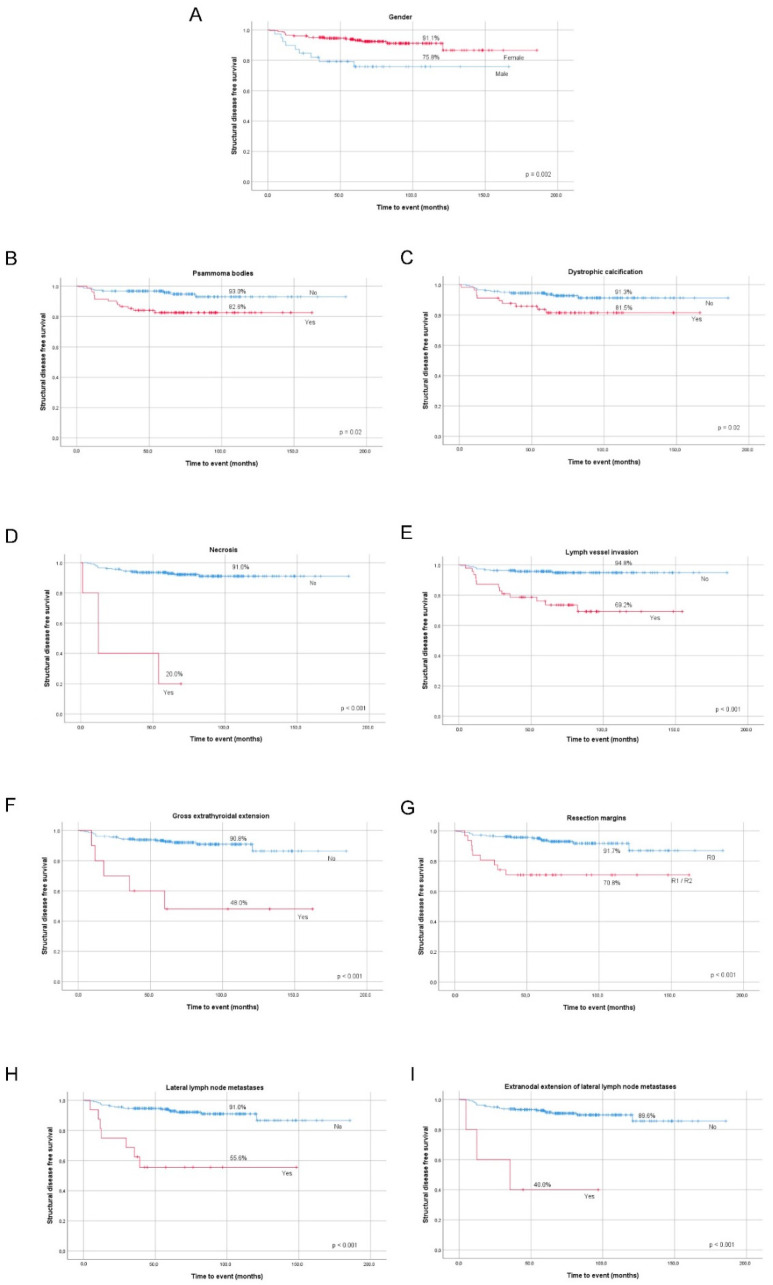
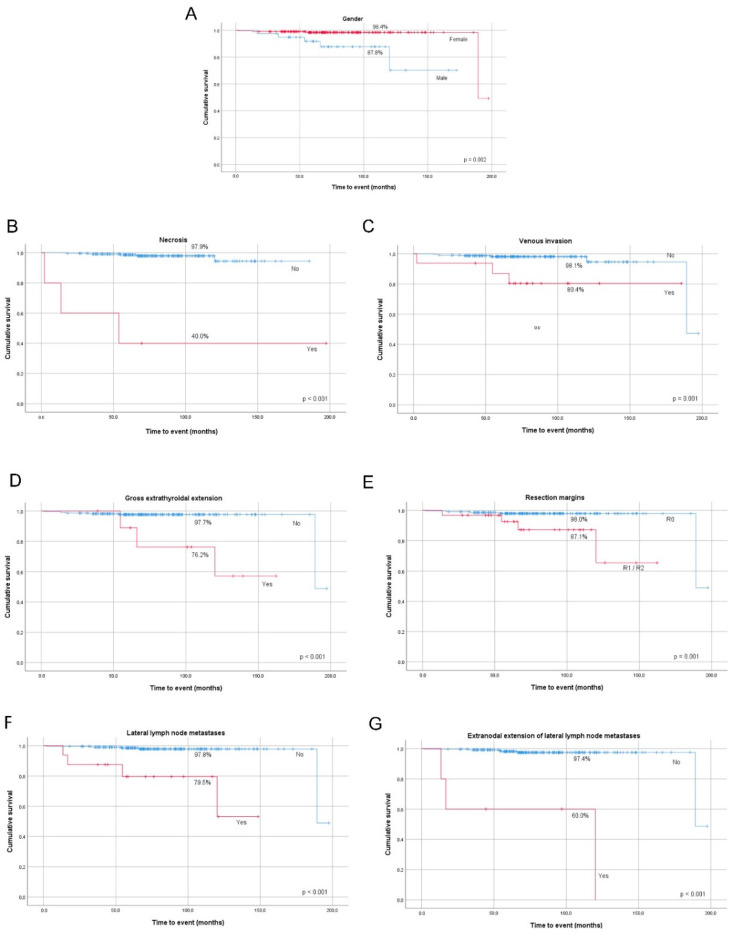
Papillary thyroid cancer (PTC) has an indolent nature and usually excellent prognosis. Some PTC clinicopathological features may contribute to the development of aggressive metastatic disease. In this work, we want to evaluate PTC clinicopathological features that are presurgical prognostic predictors of patients' outcomes and find which indicators are more adequate for tailoring surgical procedures and follow-up. We studied a series of 241 PTC patients submitted to surgery. All patients' files and histological tumor samples were reviewed. The 8th edition AJCC/UICC (American Joint Committee on Cancer/Union for International Cancer) Controlstaging system and the 2015 American Thyroid Association risk stratification system were used. Total thyroidectomy was performed in 228 patients, lymphadenectomy in 28 patients. Gross extrathyroidal extension (ETE) was present in 10 patients and 31 tumor resection margins were incomplete. Cervical lymph node metastases (LNMs) were present in 34 patients and distant metastases at diagnosis in four patients. In multivariate analysis, male gender (OR = 15.4, p = 0.015), venous invasion (OR = 16.7, p = 0.022), and lateral compartment LNM (OR = 26.7, p = 0.004) were predictors of mortality; psammoma bodies (PBs) (OR = 4.5, p = 0.008), lymph vessel invasion (OR = 6.9, p < 0.001), and gross ETE (OR = 16.1, p = 0.001) were predictors of structural disease status; male gender (OR = 2.9, p = 0.011), lymph vessel invasion (OR = 2.8, p = 0.006), and incomplete resection margins (OR = 4.6, p < 0.001) were predictors of recurrent/persistent disease. Our study supports that the factors helping to tailor patient's surgery are male gender, presence of PBs, gross ETE, and lateral compartment LNM. Together with pathological factors, lymph vessel invasion, venous invasion, necrosis, and incomplete surgical resection, should be taken into consideration regarding treatment and follow-up of patients.
Keywords: clinicopatholigical; outcomes; prognosis; thyroid cancer.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Haugen B.R., Alexander E.K., Bible K.C., Doherty G.M., Mandel S.J., Nikiforov Y.E., Pacini F., Randolph G.W., Sawka A.M., Schlumberger M., et al. American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
-
- Ferreira L.B., Lima R.T., Bastos A., Silva A.M., Tavares C., Pestana A., Rios E., Eloy C., Sobrinho-Simoes M., Gimba E.R.P., et al. OPNa Overexpression Is Associated with Matrix Calcification in Thyroid Cancer Cell Lines. Int. J. Mol. Sci. 2018;19:2990. doi: 10.3390/ijms19102990. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
