

Emerging Mechanisms of Pulmonary Vasoconstriction in SARS-CoV-2-Induced Acute Respiratory Distress Syndrome (ARDS) and Potential Therapeutic Targets
- PMID: 33138181
- PMCID: PMC7662604
- DOI: 10.3390/ijms21218081
Emerging Mechanisms of Pulmonary Vasoconstriction in SARS-CoV-2-Induced Acute Respiratory Distress Syndrome (ARDS) and Potential Therapeutic Targets
Abstract
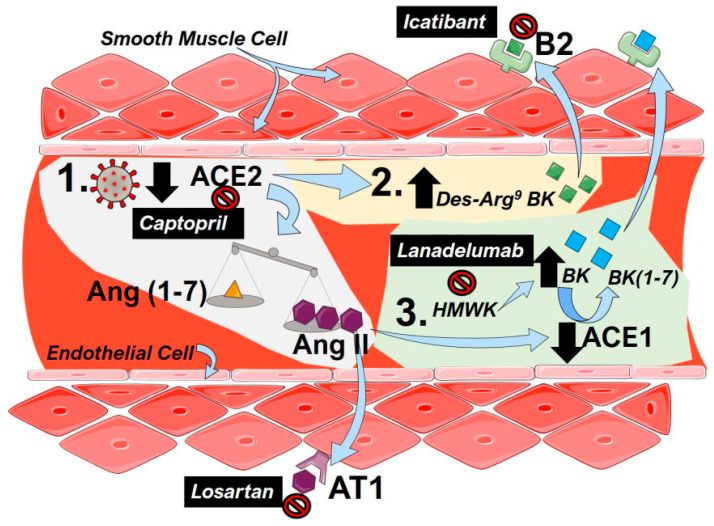
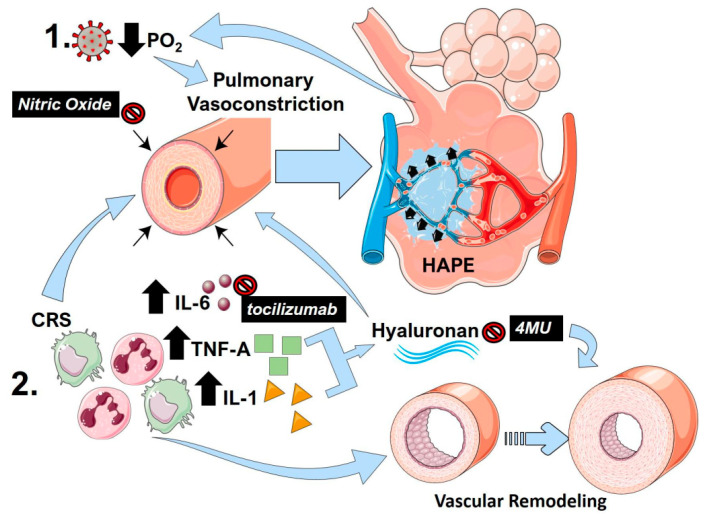
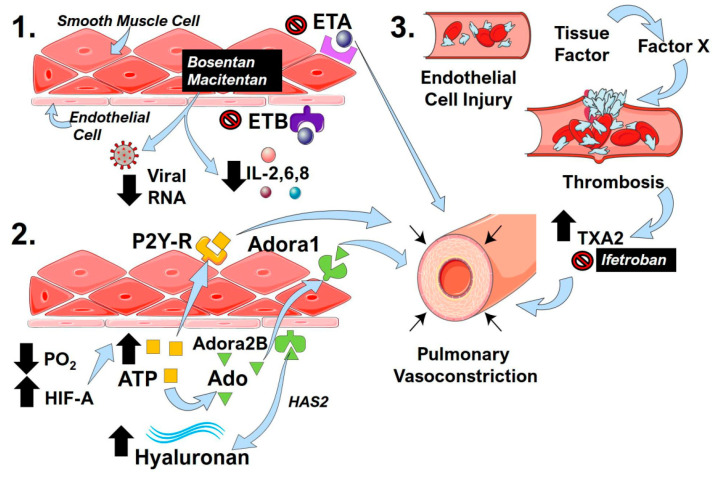
The 1918 influenza killed approximately 50 million people in a few short years, and now, the world is facing another pandemic. In December 2019, a novel coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused an international outbreak of a respiratory illness termed coronavirus disease 2019 (COVID-19) and rapidly spread to cause the worst pandemic since 1918. Recent clinical reports highlight an atypical presentation of acute respiratory distress syndrome (ARDS) in COVID-19 patients characterized by severe hypoxemia, an imbalance of the renin-angiotensin system, an increase in thrombogenic processes, and a cytokine release storm. These processes not only exacerbate lung injury but can also promote pulmonary vascular remodeling and vasoconstriction, which are hallmarks of pulmonary hypertension (PH). PH is a complication of ARDS that has received little attention; thus, we hypothesize that PH in COVID-19-induced ARDS represents an important target for disease amelioration. The mechanisms that can promote PH following SARS-CoV-2 infection are described. In this review article, we outline emerging mechanisms of pulmonary vascular dysfunction and outline potential treatment options that have been clinically tested.
Keywords: COVID-19; Kallikrein–Kinin System; acute lung injury; cytokine release storm; endothelin; hypoxic-adenosinergic response; renin angiotensin system; respiratory viral infection.
Conflict of interest statement
L.M.P.: co-investigator for the EMPACTA tocilizumab trial at Michael E.DeBakey Veterans Affairs Medical Center, Baylor College Of Medicine. S.S.: speaker for Actelion, Bayer and United therapeutics. Has accepted honorarium for speaking fees, served as a consultant for Bayer, Actelion, and United therapeutics, and accepted consultation fees. Actelion has paid for lodging and travel for presenting scientific data at an international meeting and has research grant funding from American College of Chest Physicians. H.K.-Q., R.A.T., S.P.K., and B.A. report no competing interests.
Figures
References
-
- Guo Y.-R., Cao Q.-D., Hong Z.-S., Tan Y.-Y., Chen S.-D., Jin H.-J., Tan K.-S., Wang D.-Y., Yan Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020;7:1–10. doi: 10.1186/s40779-020-00240-0. - DOI - PMC - PubMed
-
- Wu C., Chen X., Cai Y., Xia J., Zhou X., Xu S., Huang H., Zhang L., Zhou X., Du C., et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020;180:934. doi: 10.1001/jamainternmed.2020.0994. - DOI - PMC - PubMed
-
- Richardson S., Hirsch J.S., Narasimhan M., Crawford J.M., McGinn T., Davidson K.W., Barnaby D.P., Becker L.B., Chelico J.D., Cohen S.L., et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA. 2020;323:2052–2059. doi: 10.1001/jama.2020.6775. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
