

Report on planning comparison of VMAT, IMRT and helical tomotherapy for the ESCALOX-trial pre-study
- PMID: 33138837
- PMCID: PMC7607845
- DOI: 10.1186/s13014-020-01693-2
Report on planning comparison of VMAT, IMRT and helical tomotherapy for the ESCALOX-trial pre-study
Abstract
Background: The ESCALOX trial was designed as a multicenter, randomized prospective dose escalation study for head and neck cancer. Therefore, feasibility of treatment planning via different treatment planning systems (TPS) and radiotherapy (RT) techniques is essential. We hypothesized the comparability of dose distributions for simultaneous integrated boost (SIB) volumes respecting the constraints by different TPS and RT techniques.
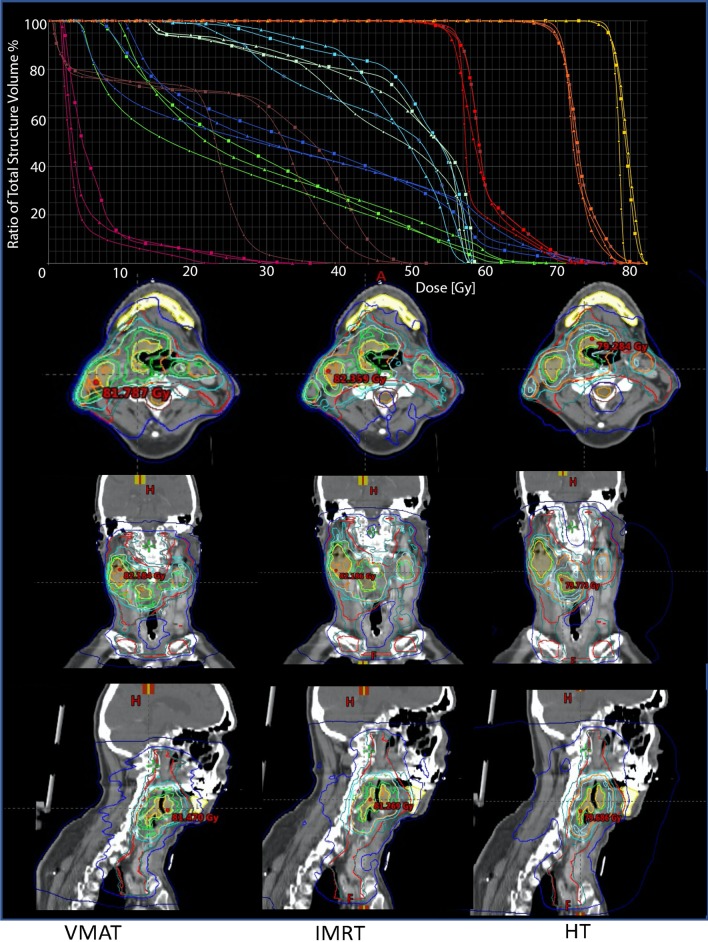
Methods: CT data sets of the first six patients (all male, mean age: 61.3 years) of the pre-study (up to 77 Gy) were used for comparison of IMRT, VMAT, and helical tomotherapy (HT). Oropharynx was the primary tumor location. Normalization of the three step SIB (77 Gy, 70 Gy, 56 Gy) was D95% = 77 Gy. Coverage (CVF), healthy tissue conformity index (HTCI), conformation number (CN), and dose homogeneity (HI) were compared for PTVs and conformation index (COIN) for parotids.
Results: All RT techniques achieved good coverage. For SIB77Gy, CVF was best for IMRT and VMAT, HT achieved highest CN followed by VMAT and IMRT. HT reached good HTCI value, and HI compared to both other techniques. For SIB70Gy, CVF was best by IMRT. HTCI favored HT, consequently CN as well. HI was slightly better for HT. For SIB56Gy, CVF resulted comparably. Conformity favors VMAT as seen by HTCI and CN. Dmean of ipsilateral and contralateral parotids favor HT.
Conclusion: Different TPS for dose escalation reliably achieved high plan quality. Despite the very good results of HT planning for coverage, conformity, and homogeneity, the TPS also achieved acceptable results for IMRT and VMAT. Trial registration ClinicalTrials.gov Identifier: NCT01212354, EudraCT-No.: 2010-021139-15. ARO: ARO 14-01.
Keywords: Combined chemoradiation therapy; Dose escalation; Head and neck cancer; Helical tomotherapy; IMRT; RT planning comparison; SIB; VMAT.
Conflict of interest statement
No one of the authors declare conflict of interest for this work.
Figures
Similar articles
-
Rotational IMRT techniques compared to fixed gantry IMRT and tomotherapy: multi-institutional planning study for head-and-neck cases.Radiat Oncol. 2011 Feb 21;6:20. doi: 10.1186/1748-717X-6-20. Radiat Oncol. 2011. PMID: 21338501 Free PMC article.
-
Dosimetric comparison of TomoDirect, helical tomotherapy, VMAT, and ff-IMRT for upper thoracic esophageal carcinoma.Med Dosim. 2019 Summer;44(2):167-172. doi: 10.1016/j.meddos.2018.05.001. Epub 2018 Jun 24. Med Dosim. 2019. PMID: 29950277
-
Whole brain radiotherapy with adjuvant or concomitant boost in brain metastasis: dosimetric comparison between helical and volumetric IMRT technique.Radiat Oncol. 2016 Apr 19;11:59. doi: 10.1186/s13014-016-0634-6. Radiat Oncol. 2016. PMID: 27094398 Free PMC article.
-
Incorporating intensity modulated total body irradiation into a Children's Oncology Group trial: Rationale, techniques, and safeguards.Pediatr Blood Cancer. 2024 Nov;71(11):e31185. doi: 10.1002/pbc.31185. Epub 2024 Aug 8. Pediatr Blood Cancer. 2024. PMID: 39118225 Review.
-
Tomotherapy for cranio-spinal irradiation.Clin Transl Radiat Oncol. 2022 Nov 11;38:96-103. doi: 10.1016/j.ctro.2022.11.003. eCollection 2023 Jan. Clin Transl Radiat Oncol. 2022. PMID: 36407491 Free PMC article. Review.
Cited by
-
Combined helical tomotherapy and Gamma Knife stereotactic radiosurgery for high-grade recurrent orbital meningioma: a case report.Front Oncol. 2023 Oct 11;13:1273465. doi: 10.3389/fonc.2023.1273465. eCollection 2023. Front Oncol. 2023. PMID: 37886178 Free PMC article.
-
Multimodal radiotherapy dose prediction using a multi-task deep learning model.Med Phys. 2024 Jun;51(6):3932-3949. doi: 10.1002/mp.17115. Epub 2024 May 6. Med Phys. 2024. PMID: 38710210 Free PMC article.
-
Development of a Monte Carlo based robustness calculation and evaluation tool.Med Phys. 2022 Jul;49(7):4780-4793. doi: 10.1002/mp.15683. Epub 2022 May 4. Med Phys. 2022. PMID: 35451087 Free PMC article.
-
Improved quality of life in head and neck cancer patients treated with modern arc radiotherapy techniques - A prospective longitudinal analysis.Front Oncol. 2024 Sep 23;14:1424034. doi: 10.3389/fonc.2024.1424034. eCollection 2024. Front Oncol. 2024. PMID: 39376987 Free PMC article.
-
Dosimetric justification for the use of volumetric modulated arc therapy in head and neck cancer-A systematic review of the literature.Laryngoscope Investig Otolaryngol. 2021 Aug 16;6(5):999-1007. doi: 10.1002/lio2.642. eCollection 2021 Oct. Laryngoscope Investig Otolaryngol. 2021. PMID: 34667842 Free PMC article. Review.
References
-
- Lauve A, Morris M, Schmidt-Ullrich R, Wu Q, Mohan R, Abayomi O, et al. Simultaneous integrated boost intensity-modulated radiotherapy for locally advanced head-and-neck squamous cell carcinomas: II—clinical results. Int J Radiat Oncol Biol Phys. 2004;60(2):374–387. doi: 10.1016/j.ijrobp.2004.03.010. - DOI - PubMed
-
- Stromberger C, Wlodarczyk W, Marnitz S, Jamil B, Budach V, Raguse JD, et al. Simultaneous integrated boost (SIB): RapidArc and tomotherapy plan comparison for unilateral and bilateral neck irradiation. Anticancer Res. 2015;35(5):2991–2997. - PubMed
-
- Fakhrian K, Oechsner M, Kampfer S, Schuster T, Molls M, Geinitz H. Advanced techniques in neoadjuvant radiotherapy allow dose escalation without increased dose to the organs at risk : planning study in esophageal carcinoma. Strahlenther Onkol. 2013;189(4):293–300. doi: 10.1007/s00066-012-0297-7. - DOI - PubMed
-
- Differding S, Sterpin E, Hermand N, Vanstraelen B, Nuyts S, de Patoul N, et al. Radiation dose escalation based on FDG-PET driven dose painting by numbers in oropharyngeal squamous cell carcinoma: a dosimetric comparison between TomoTherapy-HA and RapidArc. Radiat Oncol. 2017;12(1):59. doi: 10.1186/s13014-017-0793-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
