

Polypharmacy and emergency readmission to hospital after critical illness: a population-level cohort study
- PMID: 33138965
- PMCID: PMC8014911
- DOI: 10.1016/j.bja.2020.09.035
Polypharmacy and emergency readmission to hospital after critical illness: a population-level cohort study
Abstract
Background: Polypharmacy is common and closely linked to drug interactions. The impact of polypharmacy has not been previously quantified in survivors of critical illness who have reduced resilience to stressors. Our aim was to identify factors associated with preadmission polypharmacy and ascertain whether polypharmacy is an independent risk factor for emergency readmission to hospital after discharge from a critical illness.
Methods: A population-wide cohort study consisting of patients admitted to all Scottish general ICUs between January 1, 2011 and December 31, 2013, whom survived their ICU stay. Patients were stratified by presence of preadmission polypharmacy, defined as being prescribed five or more regular medications. The primary outcome was emergency hospital readmission within 1 yr of discharge from index hospital stay.
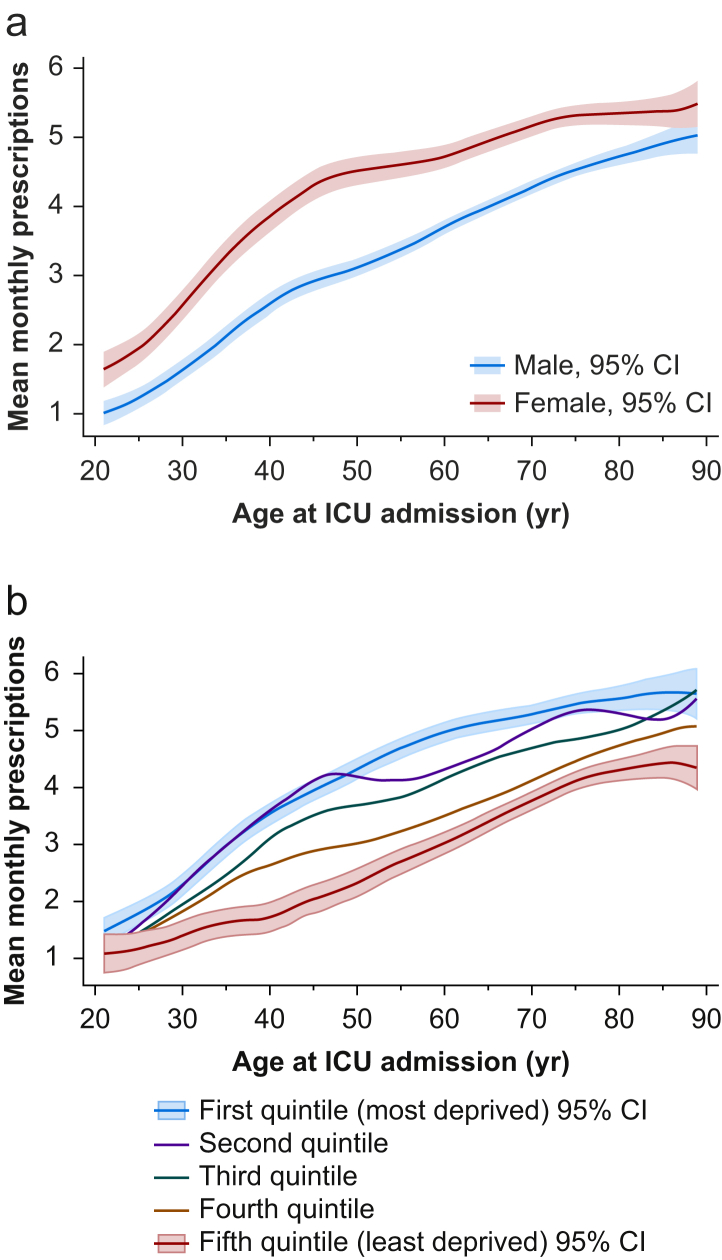
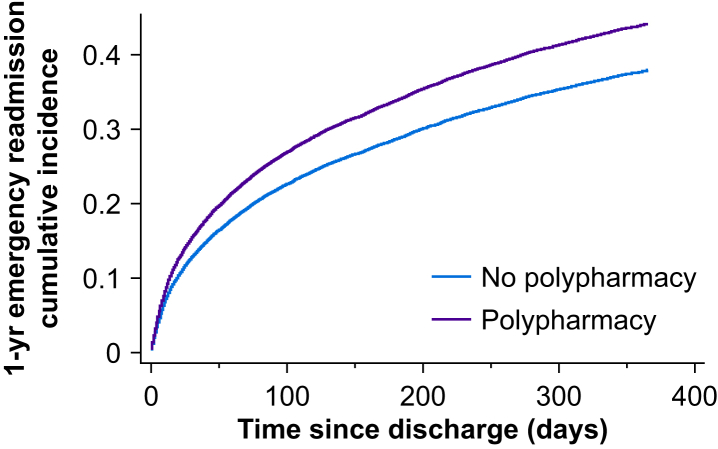
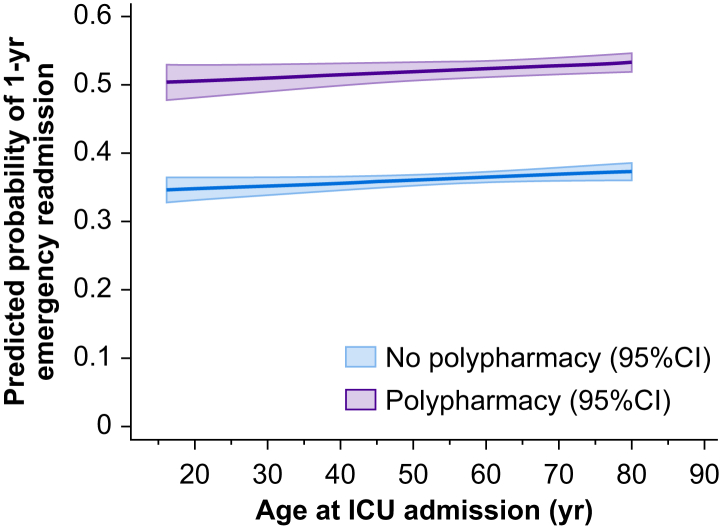
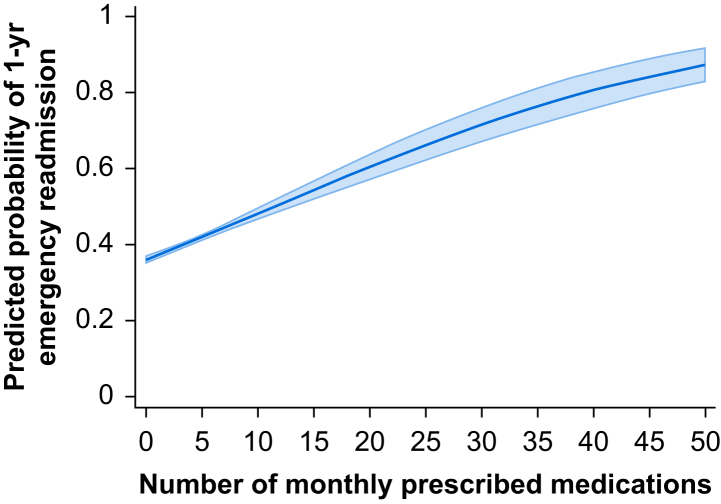
Results: Of 23 844 ICU patients, 29.9% were identified with polypharmacy (n=7138). Factors associated with polypharmacy included female sex, increasing age, and social deprivation. Emergency 1-yr hospital readmission was significantly higher in the polypharmacy cohort (51.8% vs 35.8%, P<0.001). After confounder adjustment, patients with polypharmacy had a 22% higher hazard of emergency 1-yr readmission (adjusted hazard ratio 1.22, 95% confidence interval 1.16-1.28, P<0.001). On a linear scale of polypharmacy each additional prescription conferred a 3% increase in hazard of emergency readmission by 1 yr (adjusted hazard ratio 1.03, 95% confidence interval 1.02-1.03, P<0.001).
Conclusions: This national cohort study of ICU survivors demonstrates that preadmission polypharmacy is an independent risk factor for emergency readmission. In an ever-growing era of polypharmacy, this risk factor may represent a substantial burden in the at-risk post-intensive care population.
Keywords: critical illness; drug interactions; emergency readmission; hospital readmission; intensive care; outcome; polypharmacy.
Copyright © 2020 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
References
-
- Doan J., Zakrzewski-Jakubiak H., Roy J. Prevalence and risk of potential cytochrome P450-mediated drug-drug interactions in older hospitalized patients with polypharmacy. Ann Pharmacother. 2013;47:324–332. - PubMed
-
- Uijtendaal E.V., van Harssel L.L.M., Hugenholtz G.W.K. Analysis of potential drug-drug interactions in medical intensive care unit patients. Pharmacotherapy. 2014;34:213–219. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
