

Education of pediatric surgery residents over time: Examining 15 years of case logs
- PMID: 33139026
- PMCID: PMC9618151
- DOI: 10.1016/j.jpedsurg.2020.09.038
Education of pediatric surgery residents over time: Examining 15 years of case logs
Abstract
Background/purpose: Surgical indications and techniques have changed over the last 15 years. The number of Pediatric Surgery training programs has also increased. We sought to examine the effect of these changes on resident education by examining case log data.
Methods: Accreditation Council for Graduate Medical Education (ACGME) case logs for graduating Pediatric Surgery residents were examined from 2004 to 2018. Using the summary statistics provided, linear regression analysis was conducted on each case log code and category.
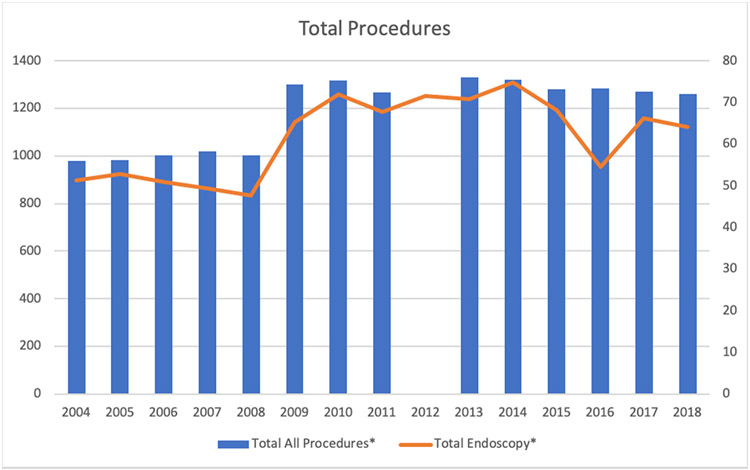
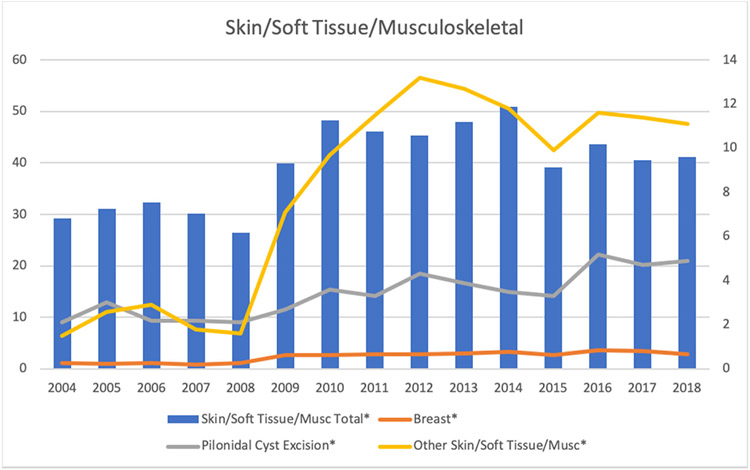
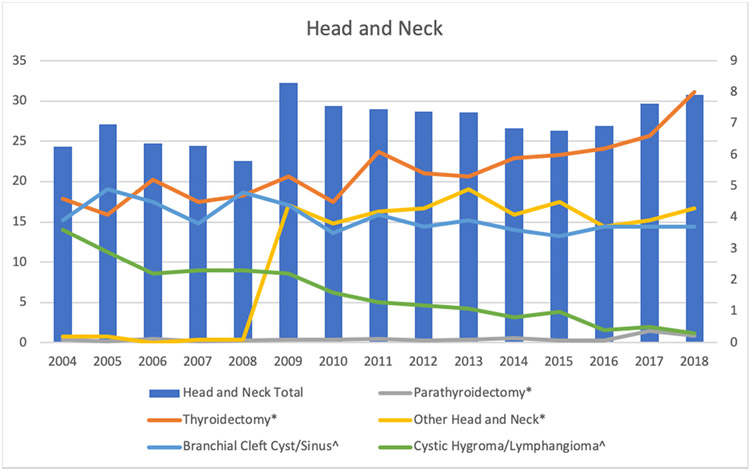
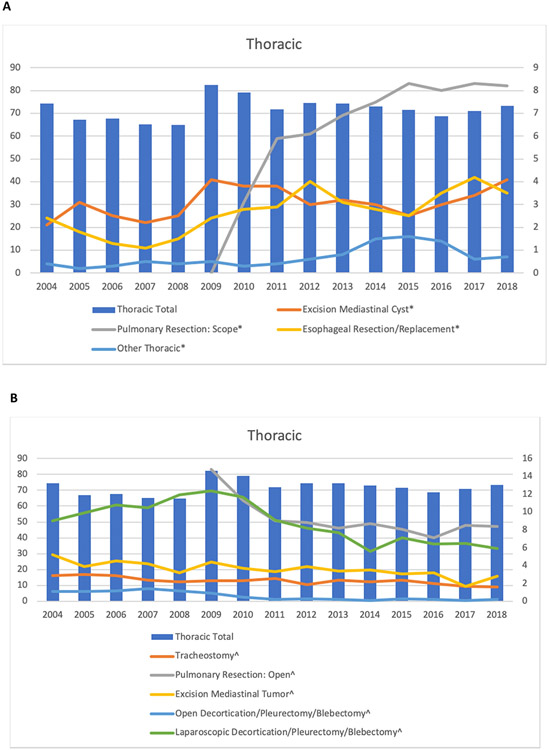
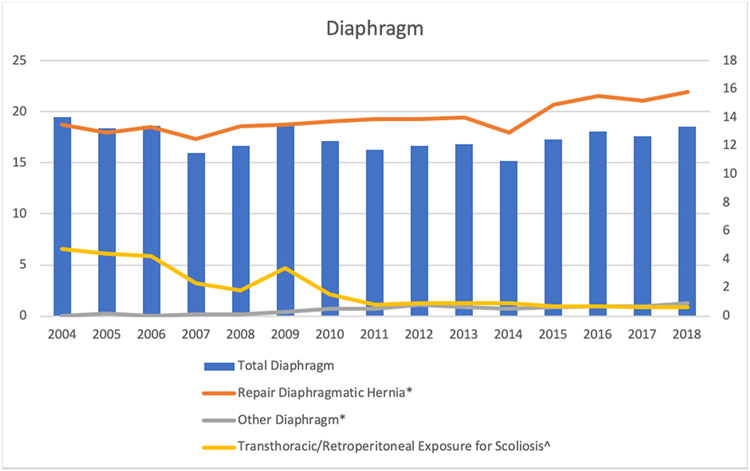
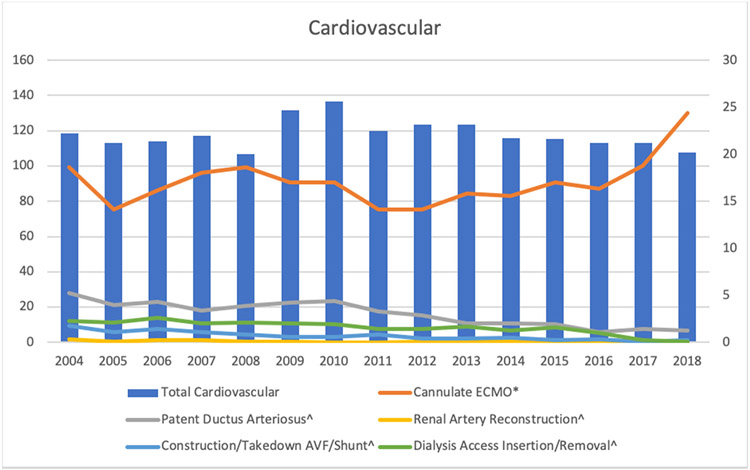
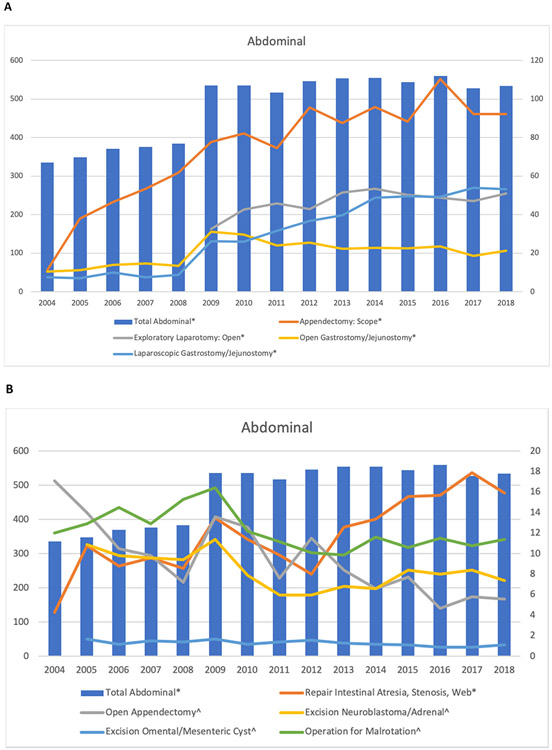
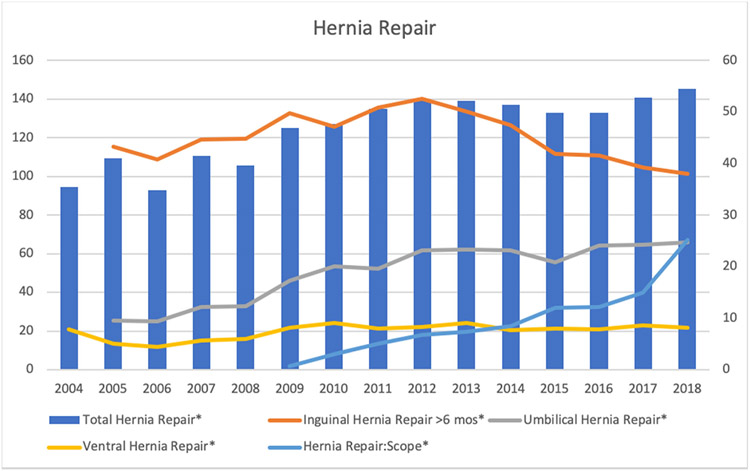
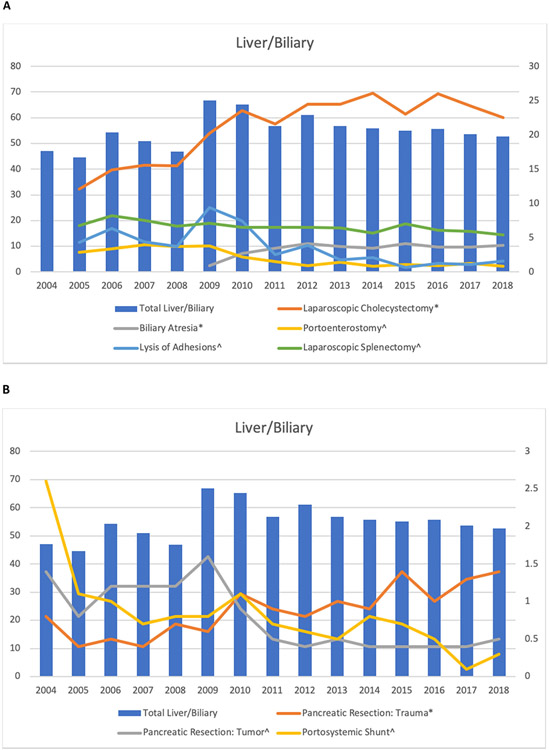
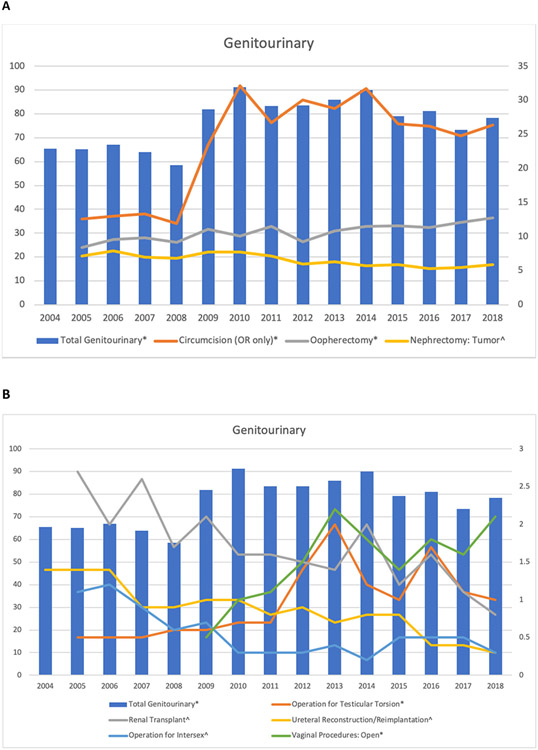
Results: In 2004, there were 24 Pediatric Surgery training programs and 24 Pediatric Surgery residents graduating with an average of 979.8 total cases logged. In 2018, there were 36 programs with 38 residents graduating with an average of 1260.2 total cases logged. Total case volume of graduating residents significantly increased over the last 15 years (p < 0.001). Significant increases were demonstrated in skin/soft tissue/musculoskeletal (p < 0.01), abdominal (p < 0.001), hernia repair (p < 0.001), genitourinary (p < 0.01), and endoscopy (p < 0.001). No significant changes were seen in the head and neck, thoracic, cardiovascular, liver/biliary, and non-operative trauma categories. No categories significantly decreased over the time period. No significant changes were seen in the number of multiple index congenital cases, including tracheoesophageal fistula/esophageal atresia repair, omphalocele, gastroschisis, choledochal cyst excision, perineal procedure for imperforate anus, and major hepatic resections for tumors. Pertinent increases in specific procedures include diaphragmatic hernia repair (p < 0.01), ECMO cannulation/decannulation(p < 0.05), thyroidectomy (p < 0.001), parathyroidectomy (p < 0.001), biliary atresia (p < 0.001), and circumcision (p < 0.001) as well as most laparoscopic abdominal procedures. Specific procedure codes with significant decreases include tracheostomy (p < 0.05), minimally invasive decortication/pleurectomy/blebectomy (p < 0.001), laparoscopic splenectomy (p < 0.001), as well as most open abdominal procedures.
Conclusion: Despite increasing numbers of Pediatric Surgery residents and training programs, the number of cases performed by each graduating resident has increased. This increase is primarily fueled by increase in abdominal, skin/soft tissue/musculoskeletal, hernia repair, genitourinary, and endoscopic cases.
Level of evidence: Level II.
Keywords: Accreditation Council for Graduate Medical Education; Pediatric surgery residency; Surgical education.
Copyright © 2020. Published by Elsevier Inc.
Conflict of interest statement
Conflict of Interest
The authors do not have any conflicts of interest to declare
Figures
Similar articles
-
Variability in gynecologic case volume of obstetrician-gynecologist residents graduating from 2009 to 2017.Am J Obstet Gynecol. 2020 Jun;222(6):617.e1-617.e8. doi: 10.1016/j.ajog.2019.11.1258. Epub 2019 Nov 22. Am J Obstet Gynecol. 2020. PMID: 31765644
-
Operative Experience of Esophageal Surgery among General Surgery Residents in the United States: An Analysis of ACGME Operative Case Logs.J Surg Educ. 2024 May;81(5):639-646. doi: 10.1016/j.jsurg.2024.01.012. Epub 2024 Mar 30. J Surg Educ. 2024. PMID: 38556439
-
Evaluating Coding Accuracy in General Surgery Residents' Accreditation Council for Graduate Medical Education Procedural Case Logs.J Surg Educ. 2016 Nov-Dec;73(6):e59-e63. doi: 10.1016/j.jsurg.2016.07.017. J Surg Educ. 2016. PMID: 27886974 Review.
-
0 + 5 Vascular Surgery Residents' Operative Experience in General Surgery: An Analysis of Operative Logs from 12 Integrated Programs.J Surg Educ. 2016 May-Jun;73(3):536-41. doi: 10.1016/j.jsurg.2015.12.010. Epub 2016 Feb 6. J Surg Educ. 2016. PMID: 26861579
-
An Analysis of Operative Experiences of Junior General Surgical Residents and Correlation With the SCORE Curriculum.J Surg Educ. 2016 Nov-Dec;73(6):e9-e13. doi: 10.1016/j.jsurg.2016.07.003. Epub 2016 Aug 8. J Surg Educ. 2016. PMID: 27515032 Review.
Cited by
-
Choosing a pediatric surgery career: affecting factors and status assessment.Pediatr Surg Int. 2024 Dec 19;41(1):33. doi: 10.1007/s00383-024-05928-1. Pediatr Surg Int. 2024. PMID: 39699668 Review.
-
Evaluation of the regional distribution of the pediatric surgery workforce and surgical load in Brazil.World J Pediatr Surg. 2023 May 16;6(2):e000522. doi: 10.1136/wjps-2022-000522. eCollection 2023. World J Pediatr Surg. 2023. PMID: 37215247 Free PMC article.
-
Development and Validation of a Realistic Neonatal Intestinal Jejunoileal Atresia Simulator for the Training of Pediatric Surgeons.Children (Basel). 2024 Sep 11;11(9):1109. doi: 10.3390/children11091109. Children (Basel). 2024. PMID: 39334641 Free PMC article.
References
-
- Sachdeva AK. The changing paradigm of residency education in surgery: a perspective from the American College of Surgeons. Am Surg. 2007;73(2):120–129. - PubMed
-
- Shin S, Britt R, Britt LD. Effect of the 80-hour work week on resident case coverage: corrected article. J Am Coll Surg. 2008;207(1):148–150. - PubMed
-
- Shin S, Britt R, Doviak M, Britt LD. The impact of the 80-hour work week on appropriate resident case coverage. J Surg Res. 2010;162(1):33–36. - PubMed
-
- Fairfax LM, Christmas AB, Green JM, Miles WS, Sing RF. Operative experience in the era of duty hour restrictions: is broad-based general surgery training coming to an end? Am Surg. 2010;76(6):578–582. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
