

Tumor Mutational Burden as a Predictive Biomarker in Solid Tumors
- PMID: 33139244
- PMCID: PMC7710563
- DOI: 10.1158/2159-8290.CD-20-0522
Tumor Mutational Burden as a Predictive Biomarker in Solid Tumors
Abstract
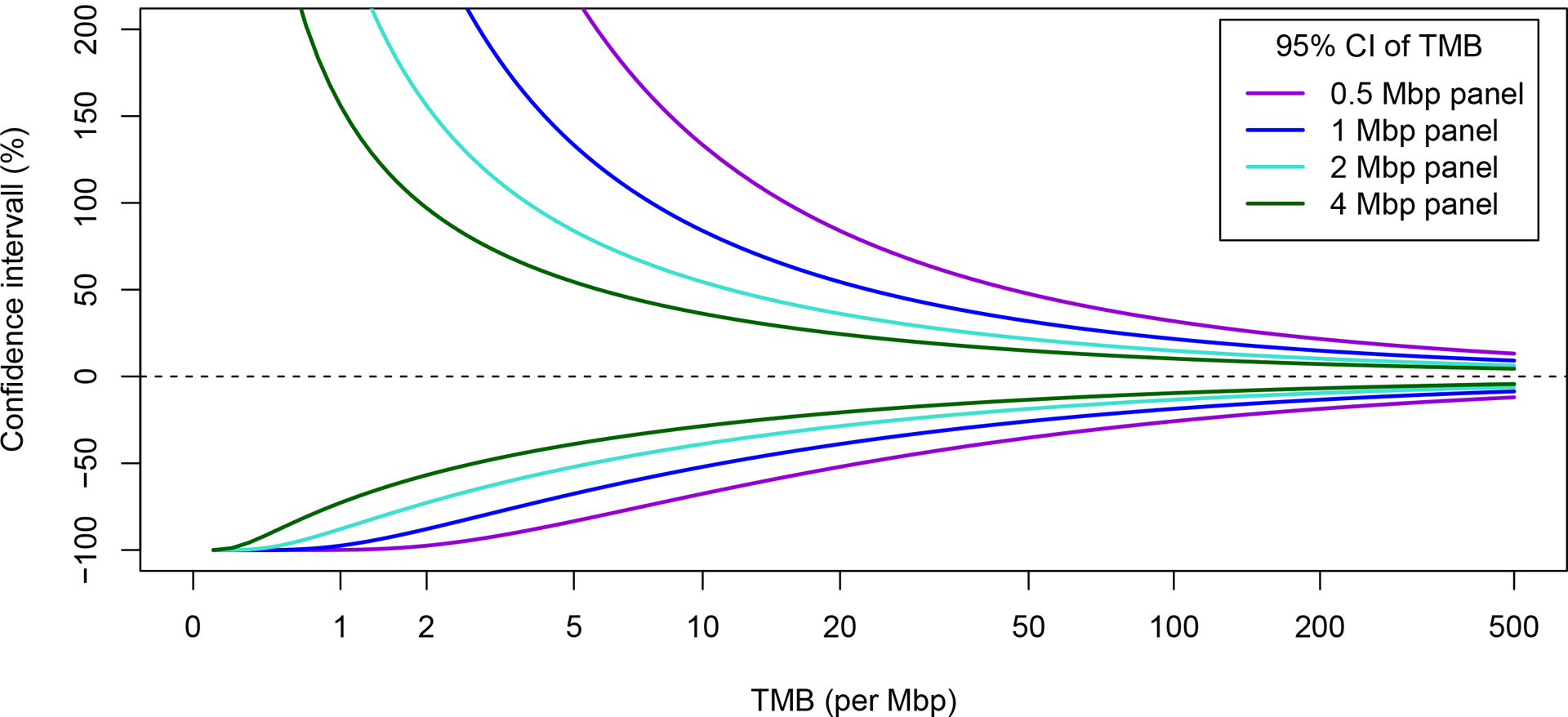
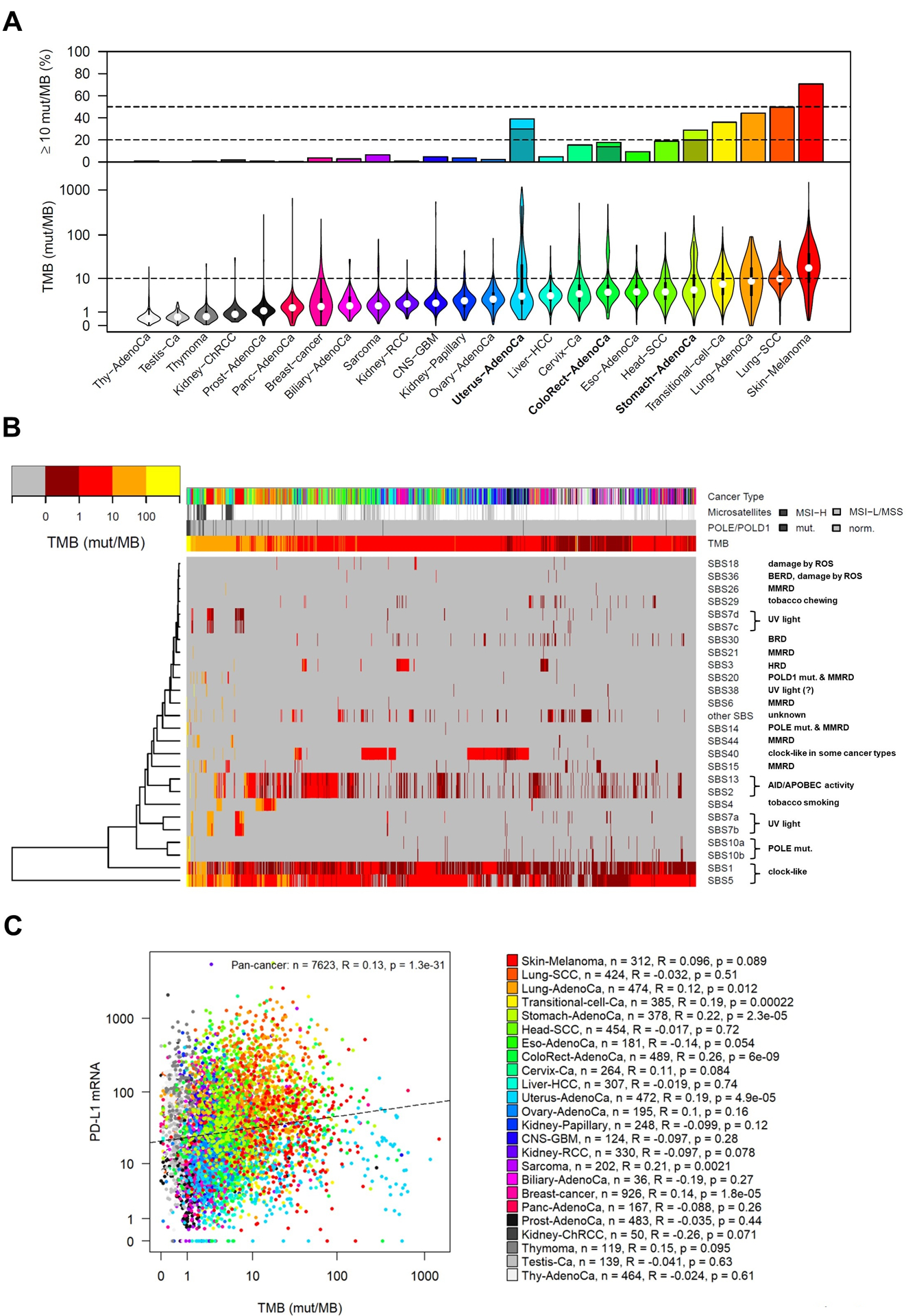
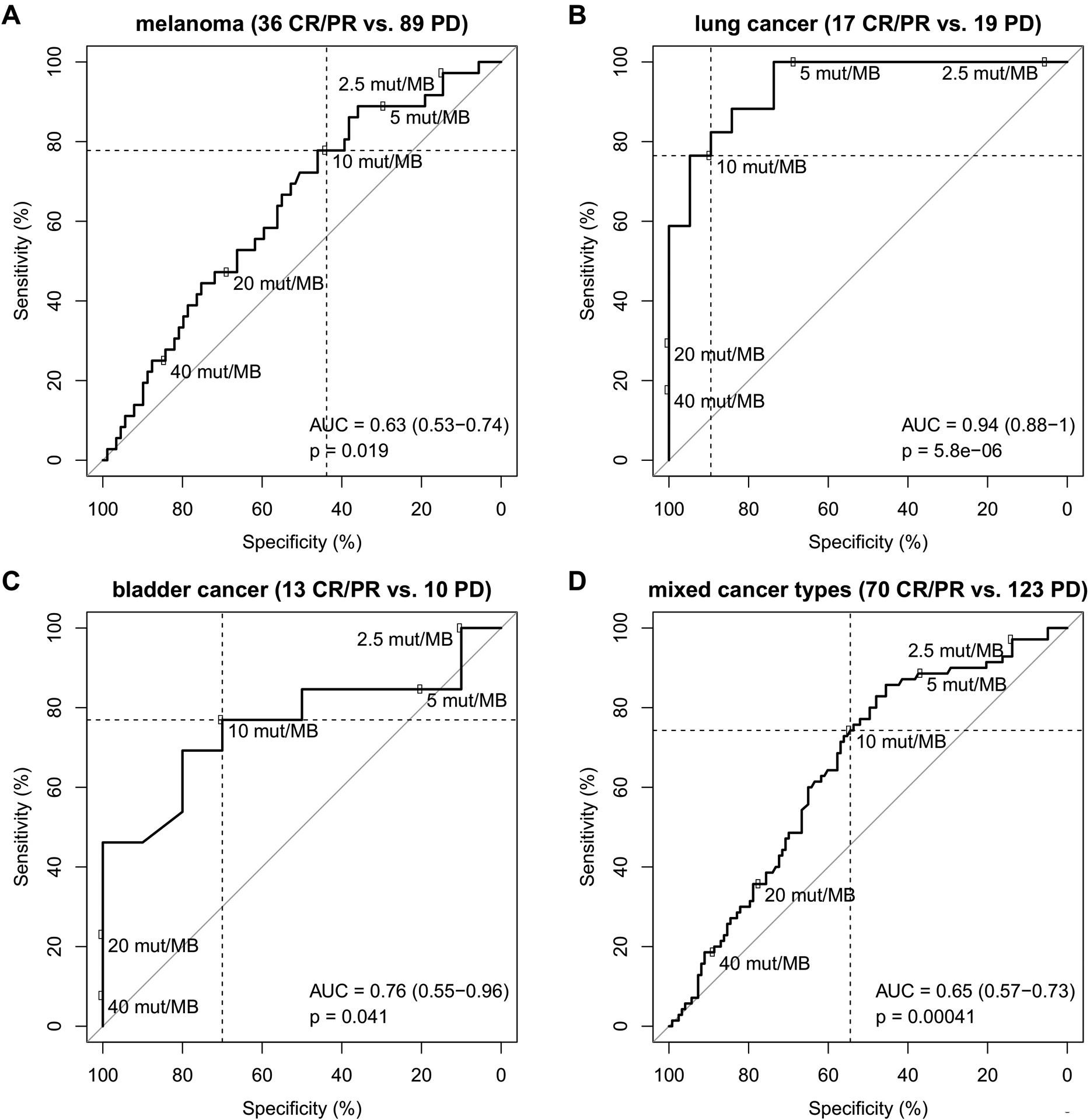
Tumor mutational burden (TMB), defined as the number of somatic mutations per megabase of interrogated genomic sequence, varies across malignancies. Panel sequencing-based estimates of TMB have largely replaced whole-exome sequencing-derived TMB in the clinic. Retrospective evidence suggests that TMB can predict the efficacy of immune checkpoint inhibitors, and data from KEYNOTE-158 led to the recent FDA approval of pembrolizumab for the TMB-high tumor subgroup. Unmet needs include prospective validation of TMB cutoffs in relationship to tumor type and patient outcomes. Furthermore, standardization and harmonization of TMB measurement across test platforms are important to the successful implementation of TMB in clinical practice. SIGNIFICANCE: Evaluation of TMB as a predictive biomarker creates the need to harmonize panel-based TMB estimation and standardize its reporting. TMB can improve the predictive accuracy for immunotherapy outcomes, and has the potential to expand the candidate pool of patients for treatment with immune checkpoint inhibitors.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
