

COVID-19-associated gastrointestinal and liver injury: clinical features and potential mechanisms
- PMID: 33139693
- PMCID: PMC7605138
- DOI: 10.1038/s41392-020-00373-7
COVID-19-associated gastrointestinal and liver injury: clinical features and potential mechanisms
Abstract
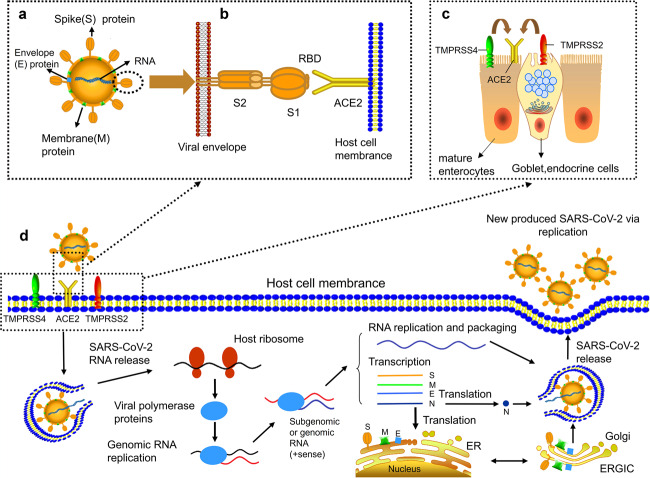
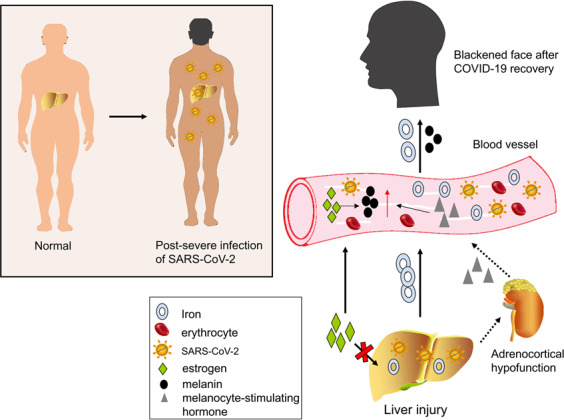
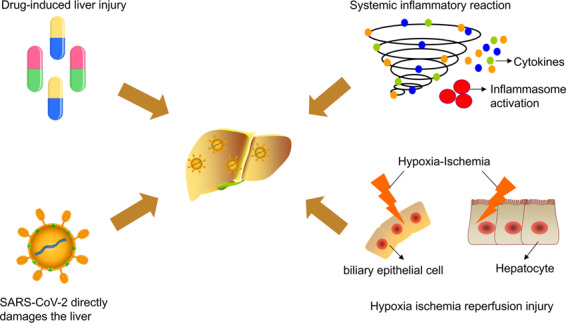
Coronavirus disease-2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The infection is spreading globally and poses a huge threat to human health. Besides common respiratory symptoms, some patients with COVID-19 experience gastrointestinal symptoms, such as diarrhea, nausea, vomiting, and loss of appetite. SARS-CoV-2 might infect the gastrointestinal tract through its viral receptor angiotensin-converting enzyme 2 (ACE2) and there is increasing evidence of a possible fecal-oral transmission route. In addition, there exist multiple abnormalities in liver enzymes. COVID-19-related liver injury may be due to drug-induced liver injury, systemic inflammatory reaction, and hypoxia-ischemia reperfusion injury. The direct toxic attack of SARS-CoV-2 on the liver is still questionable. This review highlights the manifestations and potential mechanisms of gastrointestinal and hepatic injuries in COVID-19 to raise awareness of digestive system injury in COVID-19.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. Coronavirus disease (COVID-19) pandemic, 2020. https://www.who.int/health-topics/coronavirus#tab=tab_1 (2020).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
