

Extracorporeal life support for adults with acute respiratory distress syndrome
- PMID: 33140180
- PMCID: PMC7605473
- DOI: 10.1007/s00134-020-06290-1
Extracorporeal life support for adults with acute respiratory distress syndrome
Abstract
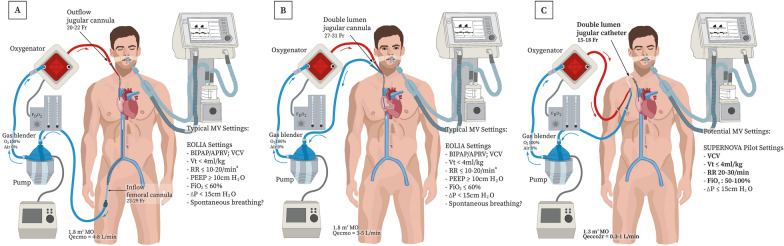
Extracorporeal life support (ECLS) can support gas exchange in patients with the acute respiratory distress syndrome (ARDS). During ECLS, venous blood is drained from a central vein via a cannula, pumped through a semipermeable membrane that permits diffusion of oxygen and carbon dioxide, and returned via a cannula to a central vein. Two related forms of ECLS are used. Venovenous extracorporeal membrane oxygenation (ECMO), which uses high blood flow rates to both oxygenate the blood and remove carbon dioxide, may be considered in patients with severe ARDS whose oxygenation or ventilation cannot be maintained adequately with best practice conventional mechanical ventilation and adjunctive therapies, including prone positioning. Extracorporeal carbon dioxide removal (ECCO2R) uses lower blood flow rates through smaller cannulae and provides substantial CO2 elimination (~ 20-70% of total CO2 production), albeit with marginal improvement in oxygenation. The rationale for using ECCO2R in ARDS is to facilitate lung-protective ventilation by allowing a reduction of tidal volume, respiratory rate, plateau pressure, driving pressure and mechanical power delivered by the mechanical ventilator. This narrative review summarizes physiological concepts related to ECLS, as well as the rationale and evidence supporting ECMO and ECCO2R for the treatment of ARDS. It also reviews complications, limitations, and the ethical dilemmas that can arise in treating patients with ECLS. Finally, it discusses future key research questions and challenges for this technology.
Keywords: Acute respiratory failure; Extracorporeal membrane oxygenation; Mechanical ventilation; Outcome.
Conflict of interest statement
AC reports grants from Getinge, personal fees from Getinge, Baxter and Xenios outside the submitted work. AC is also the recent past president of the EuroELSO organization and a member of the executive and scientific committees for ECMONet. MS reported personal fees from Getinge, Drager, and Xenios, outside the submitted work. MS is also member of the Data Committee for ECMONet. CH is a member of the steering and scientific committees for ECMONet. EF reports personal fees from ALung Technologies, Fresenius Medical Care, Getinge, and MC3 Cardiopulmonary outside the submitted work. NF reports consulting fees from Getinge and Xenios. NF is a member of the executive and scientific committees for ECMONet. JF is current president of Asia Pacific ELSO, Exec of ECMOnet, and has received grant funding from Getinge, Xenios, Drager and CSL. He is co-founder of BiVACOR (mechanical support device). He declares no personal fees. SJ reports receiving consulting fees from Drager, Fresenius-Xenios, Baxter, Medtronic, and Fisher & Paykel. AP reports perrsonal fees for consulting/lectures from Maquet, Xenios, Baxter, and Boehringer Ingelheim. AS is on the medical advisory boards for Baxter and Xenios. Hs is Chair of the Scientific Committee of the International ECMO Network (ECMONet). DB receives research support from ALung Technologies. He has been on the medical advisory boards for Baxter, Abiomed, Xenios and Hemovent. DB is also the President-elect of the Extracorporeal Life Support Organization (ELSO) and the Chair of the Executive Committee of the International ECMO Network (ECMONet). The other authors declare that they have no conflicts of interest related to the purpose of this manuscript.
Figures
References
-
- Acute Respiratory Distress Syndrome Network; Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301–1308 - PubMed
