

Clinical strategies for implementing lung and diaphragm-protective ventilation: avoiding insufficient and excessive effort
- PMID: 33140181
- PMCID: PMC7605467
- DOI: 10.1007/s00134-020-06288-9
Clinical strategies for implementing lung and diaphragm-protective ventilation: avoiding insufficient and excessive effort
Abstract
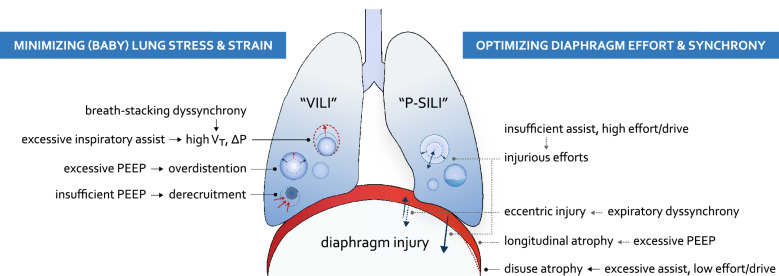
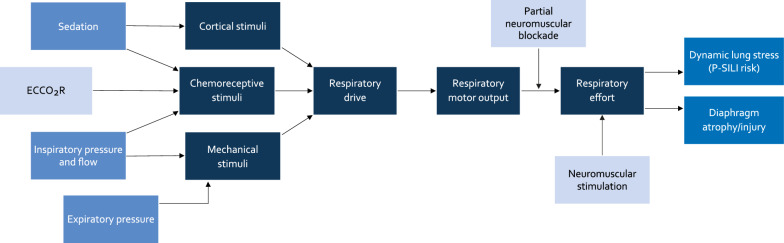
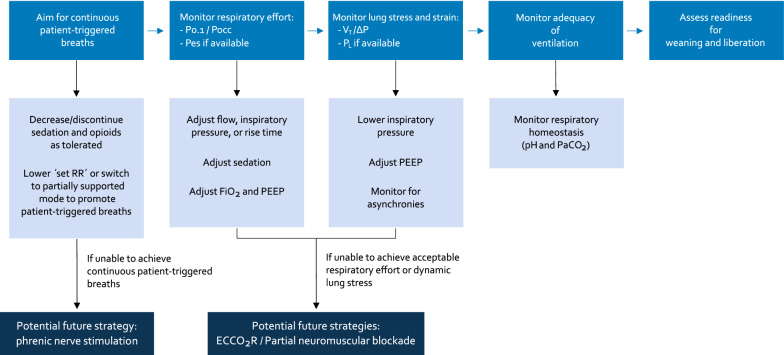
Mechanical ventilation may have adverse effects on both the lung and the diaphragm. Injury to the lung is mediated by excessive mechanical stress and strain, whereas the diaphragm develops atrophy as a consequence of low respiratory effort and injury in case of excessive effort. The lung and diaphragm-protective mechanical ventilation approach aims to protect both organs simultaneously whenever possible. This review summarizes practical strategies for achieving lung and diaphragm-protective targets at the bedside, focusing on inspiratory and expiratory ventilator settings, monitoring of inspiratory effort or respiratory drive, management of dyssynchrony, and sedation considerations. A number of potential future adjunctive strategies including extracorporeal CO2 removal, partial neuromuscular blockade, and neuromuscular stimulation are also discussed. While clinical trials to confirm the benefit of these approaches are awaited, clinicians should become familiar with assessing and managing patients' respiratory effort, based on existing physiological principles. To protect the lung and the diaphragm, ventilation and sedation might be applied to avoid excessively weak or very strong respiratory efforts and patient-ventilator dysynchrony.
Keywords: Diaphragm weakness; Lung injury; Mechanical ventilation’; Respiratory effort.
Conflict of interest statement
EG is supported by an Early Career Investigator award from the Canadian Institutes of Health Research (AR7-162822). He has received research support in the form of equipment from Getinge and Timpel and personal fees from Getinge. SJ reports receiving consulting fees from Drager, Medtronic, Baxter, Fresenius Medical and Fisher & Paykel. TM received personal fees from Fisher and Paykel, Drager, Mindray, Braun outside of the submitted work. LB’s laboratory reports grants from Medtronic Covidien, grants and non-financial support from Fisher Paykel, non-financial support from Air Liquide, non-financial support from Sentec, non-financial support from Philips, a patent with General Electric, outside the submitted work. LH received research grants from Liberate Medical and Orion Pharma, and travel and speakers fee from Getinge and Orion Pharma.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
