

Trend and status of out-of-pocket payments for healthcare in Iran: equity and catastrophic effect
- PMID: 33140214
- PMCID: PMC7606373
- DOI: 10.1186/s42506-020-00055-w
Trend and status of out-of-pocket payments for healthcare in Iran: equity and catastrophic effect
Abstract
Background: Equity in the distribution of health care resources and mitigating the risk of out-of-pocket (OOP) catastrophic healthcare expenditures (CHE) are the major objectives of the health system of a country. This study aims to measure equity in OOP payments for healthcare and the incidence of CHE among Iranian households over time.
Methods: This retrospective cross-sectional study utilized data extracted from the household income and expenditure survey (HIES) of Iran, collected by the Statistical Center of Iran. The analysis included a total of 174,341 households' five yearly data of 6 years starting from 1991 to 2017. Kakwani progressivity index (KPI) was used to measure the equity in OOP payment for each year and examine the households' incidence of CHE at 20%, 30%, and 40% of their capacities to pay (CTP). The trend series regression analysis was used to examine the trend in the KPI and the incidence of the CHE over time.
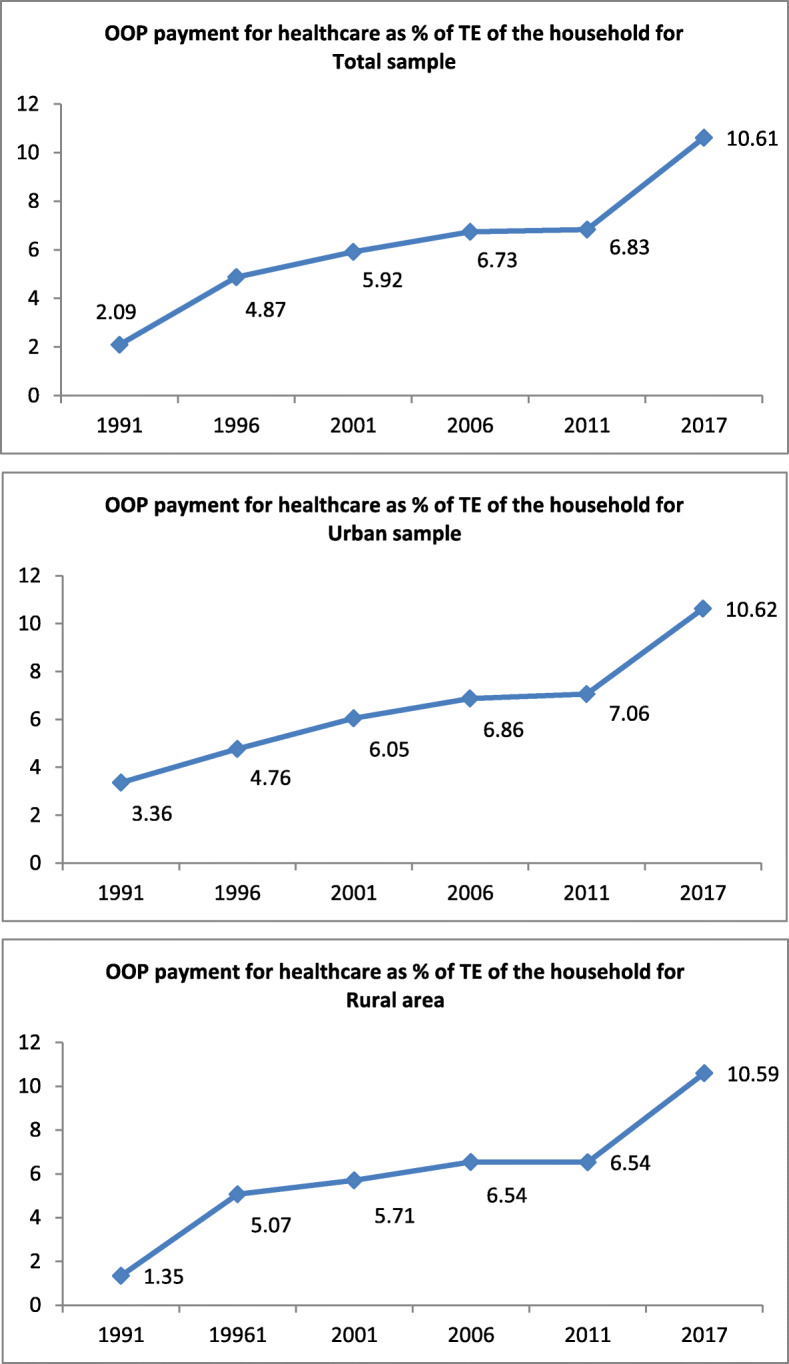
Results: The findings indicated that the households' expenditure on health out of their monthly budgets for the years 1991 and 2017 were 2.1% and 10.1%, respectively. The KPI for the OOP payment was negative for all 6-year observations (1991 = - 0.680; 1996 = - 0.608; 2001 = - 0.554; 2006 = - 0.265; 2011 = - 0.225, and 2017 = - 0.207), indicating that the OOP payments for healthcare are regressive and more concentrated among the socioeconomically disadvantaged households. There was a statistically significant (p = 0.003) increase in the KPI (i.e., decline in the regressivity) over time. The incidence of the CHE (1.12, 1.93, and 3.71%) in 1991 at the CTP levels of 20%, 30%, and 40% was lower than the incidence at the corresponding levels of CTP (5.26, 10.88, and 22.16) in 2017. The findings of the time-series regression indicated a statistically significant (p < 0.05) increase in the incidence of the CHE at the 20%, 30%, and 40% levels of the households' CTP.
Conclusions: The current study demonstrated that OOP payment as a source of healthcare funding in Iran is inequitable. While the use of interventions such as the prepaid and publicly funded programs may contribute to the reduction of CHE and improvement of equity in healthcare financing, further inequality analyses in the incidence of the CHE among households and its main determinants can contribute to evidence-informed planning to reduce the CHE in the context.
Keywords: Catastrophic healthcare expenditure; Financing personal; Health disparities; Health equity; Health expenditure; Kakwani progressivity index; Out-of-pocket payments.
Conflict of interest statement
The authors declare that there are no competing interests.
Figures
Similar articles
-
The Variations in Catastrophic and Impoverishing Health Expenditures, and Its Determinants in Iran: A Scoping Review.Med J Islam Repub Iran. 2023 Apr 26;37:44. doi: 10.47176/mjiri.37.44. eCollection 2023. Med J Islam Repub Iran. 2023. PMID: 37426477 Free PMC article.
-
The Effect of Iran Health Transformation Plan on Equity in Health Financing: A Systematic Review.Iran J Public Health. 2023 Sep;52(9):1844-1854. doi: 10.18502/ijph.v52i9.13567. Iran J Public Health. 2023. PMID: 38033830 Free PMC article. Review.
-
Equity in Out-of-Pocket Payments for Healthcare Services: Evidence from Malaysia.Int J Environ Res Public Health. 2022 Apr 8;19(8):4500. doi: 10.3390/ijerph19084500. Int J Environ Res Public Health. 2022. PMID: 35457364 Free PMC article.
-
Household financial burden associated with out-of-pocket payments for healthcare in Iran: insights from a cross-sectional survey.BMC Health Serv Res. 2024 Sep 13;24(1):1062. doi: 10.1186/s12913-024-11477-z. BMC Health Serv Res. 2024. PMID: 39272081 Free PMC article.
-
Catastrophic Health Expenditure among Iranian Households: Evidence from the COVID-19 Era.Med J Islam Repub Iran. 2024 May 1;38:49. doi: 10.47176/mjiri.38.49. eCollection 2024. Med J Islam Repub Iran. 2024. PMID: 39399604 Free PMC article.
Cited by
-
The Variations in Catastrophic and Impoverishing Health Expenditures, and Its Determinants in Iran: A Scoping Review.Med J Islam Repub Iran. 2023 Apr 26;37:44. doi: 10.47176/mjiri.37.44. eCollection 2023. Med J Islam Repub Iran. 2023. PMID: 37426477 Free PMC article.
-
Exploring dental and medicine health expenditures in Iran: financial protection and inequality analysis.J Health Popul Nutr. 2025 Mar 26;44(1):87. doi: 10.1186/s41043-025-00828-z. J Health Popul Nutr. 2025. PMID: 40140951 Free PMC article.
-
Did health reform improve financial protection for disadvantaged groups in Ecuador? A socio-economic inequality assessment of catastrophic health expenditures 2006-2014.BMJ Open. 2025 Jul 30;15(7):e100522. doi: 10.1136/bmjopen-2025-100522. BMJ Open. 2025. PMID: 40738632 Free PMC article.
-
The Effect of Iran Health Transformation Plan on Equity in Health Financing: A Systematic Review.Iran J Public Health. 2023 Sep;52(9):1844-1854. doi: 10.18502/ijph.v52i9.13567. Iran J Public Health. 2023. PMID: 38033830 Free PMC article. Review.
-
Equity in Out-of-Pocket Payments for Healthcare Services: Evidence from Malaysia.Int J Environ Res Public Health. 2022 Apr 8;19(8):4500. doi: 10.3390/ijerph19084500. Int J Environ Res Public Health. 2022. PMID: 35457364 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
