

Targeted Next-Generation Sequencing Analysis for Recurrence in Early-Stage Lung Adenocarcinoma
- PMID: 33140254
- PMCID: PMC8184531
- DOI: 10.1245/s10434-020-09276-x
Targeted Next-Generation Sequencing Analysis for Recurrence in Early-Stage Lung Adenocarcinoma
Abstract
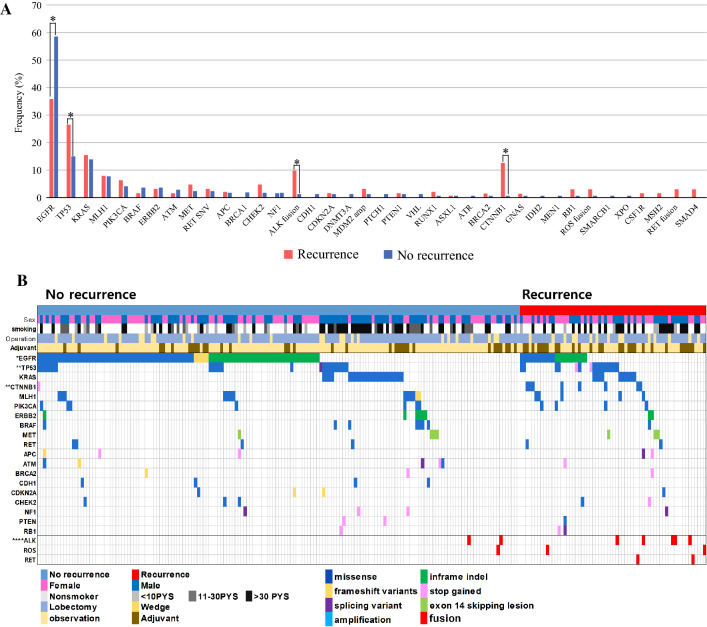
Background: Despite surgical resection, early lung adenocarcinoma has a recurrence rate of 20-50%. No clear predictive markers for recurrence of early lung adenocarcinoma are available. Targeted next-generation sequencing (NGS) is rarely used to identify recurrence-related genes. We aimed to identify genetic alterations that can predict recurrence, by comparing the molecular profiles of patient groups with and without recurrence.
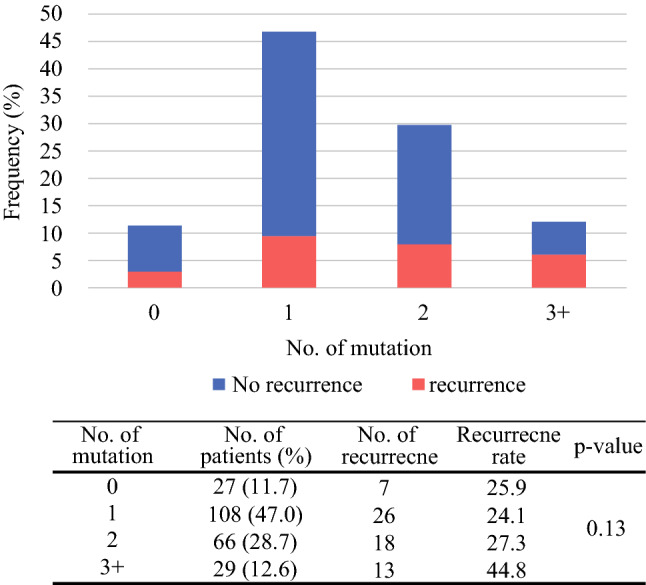
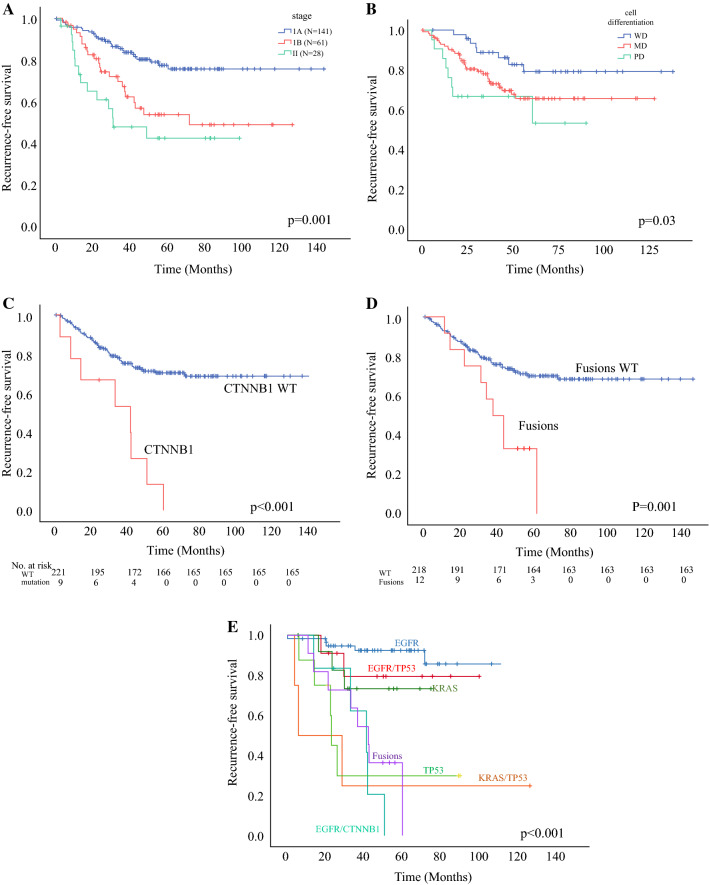
Methods: Tissues from 230 patients with resected stage I-II lung adenocarcinoma (median follow-up: 49 months) were analyzed via targeted NGS for 207 cancer-related genes. The recurrence-free survival according to the number and type of mutation was estimated using the Kaplan-Meier method. Independent predictive biomarkers related to recurrence were identified using the Cox proportional hazards model.
Results: Recurrence was observed in 64 patients (27.8%). In multivariate analysis adjusted for age, sex, smoking history, stage, surgical mode, and visceral pleural invasion, the CTNNB1 mutation and fusion genes (ALK, ROS1, RET) were negative prognostic factors for recurrence in early-stage lung adenocarcinoma (HR 4.47, p = 0.001; HR 2.73, p = 0.009). EGFR mutation was a favorable factor (HR 0.51, p = 0.016), but the CTNNB1/EGFR co-mutations were negative predictors (HR 19.2, p < 0.001). TP53 mutation was a negative predictor compared with EGFR mutation for recurrence (HR 5.24, p = 0.02).
Conclusions: Targeted NGS can provide valuable information to predict recurrence and identify patients at high recurrence risk, facilitating selection of the treatment strategy among close monitoring and adjuvant-targeted therapy. Larger datasets are required to validate these findings.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Maeda R, Yoshida J, Ishii G, Hishida T, Nishimura M, Nagai K. Risk factors for tumor recurrence in patients with early-stage (stage I and II) non-small cell lung cancer: patient selection criteria for adjuvant chemotherapy according to the seventh edition TNM classification. CHEST J. 2011;140(6):1494–1502. doi: 10.1378/chest.10-3279. - DOI - PubMed
-
- Nadal E, Chen G, Prensner JR, et al. KRAS-G12C mutation is associated with poor outcome in surgically resected lung adenocarcinoma. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. 2014;9(10):1513–1522. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
